

Background: The ribcage is formed by a collection of twelve (12) ribs of various lengths, locations and compositions. The first seven (7) ribs are called the true ribs because they run between the spine to the sternum through a direct curvilinear connection. Ribs #s 8, 9 and 10 are called the false ribs because they are indirectly connected to the sternum through long curved cartilaginous connections to the seventh rib. Lastly the floating ribs are #s 11 and 12 because they have no sternal connection at all.
Besides the midline sternum and the shape of the adjoining upper chest, the other distinguishing ribcage feature is that of the subcostal region. Everyone knows this ribcage area well because you can put your hand up under it and even move it a bit. This is formed by the cartilaginous connections of the false ribs as they come around and upward to connect to rib #7. It is somewhat mobile because of its cartilage composition and can create its own aesthetic issues if it is too prominent.
One potential cause of an acquired subcostal ribcage protrusion deformity is trauma. Like all ribs, with the exception of #s1, 11 and 12, there is a bone-cartilage junction. (costochondral junction) This junction can be prone to separation from trauma as it is the ‘weak’ link along the entire length of the rib. Such costochondral disruptions can create a change in the subcostal shape.
 Case Study: This middle-aged male developed a right subcostal protrusion after a traumatic event when he was struck by an object on that side of his chest. It was presumed that this caused a separation of the costochondral junction of ribs #s 8 and 9 and a resultant deformation of the subcostal ribcage.
Case Study: This middle-aged male developed a right subcostal protrusion after a traumatic event when he was struck by an object on that side of his chest. It was presumed that this caused a separation of the costochondral junction of ribs #s 8 and 9 and a resultant deformation of the subcostal ribcage.
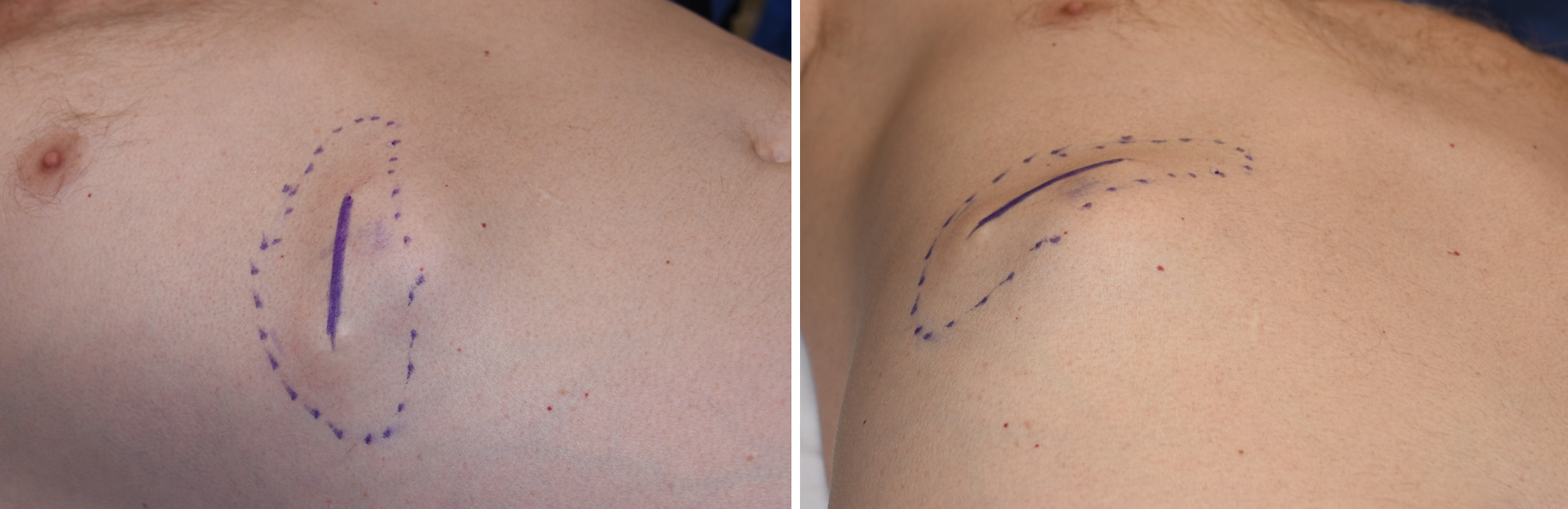
 Under general anesthesia a 4 cm skin incision was made directly over the ribcage protrusion. The rectus muscle was vertically split for access to the protruding cartilaginous ribs. The protruding rib portion was shaved down with a large scalpel blade until the protrusion was eliminated and only a thin layer of cartilage was left. Some shaving was also carried over onto rib #10. After injection of Marcaine local anesthetic into the muscle and intercostal nerves, the muscle and skin were closed with dissolvable sutures.
Under general anesthesia a 4 cm skin incision was made directly over the ribcage protrusion. The rectus muscle was vertically split for access to the protruding cartilaginous ribs. The protruding rib portion was shaved down with a large scalpel blade until the protrusion was eliminated and only a thin layer of cartilage was left. Some shaving was also carried over onto rib #10. After injection of Marcaine local anesthetic into the muscle and intercostal nerves, the muscle and skin were closed with dissolvable sutures.
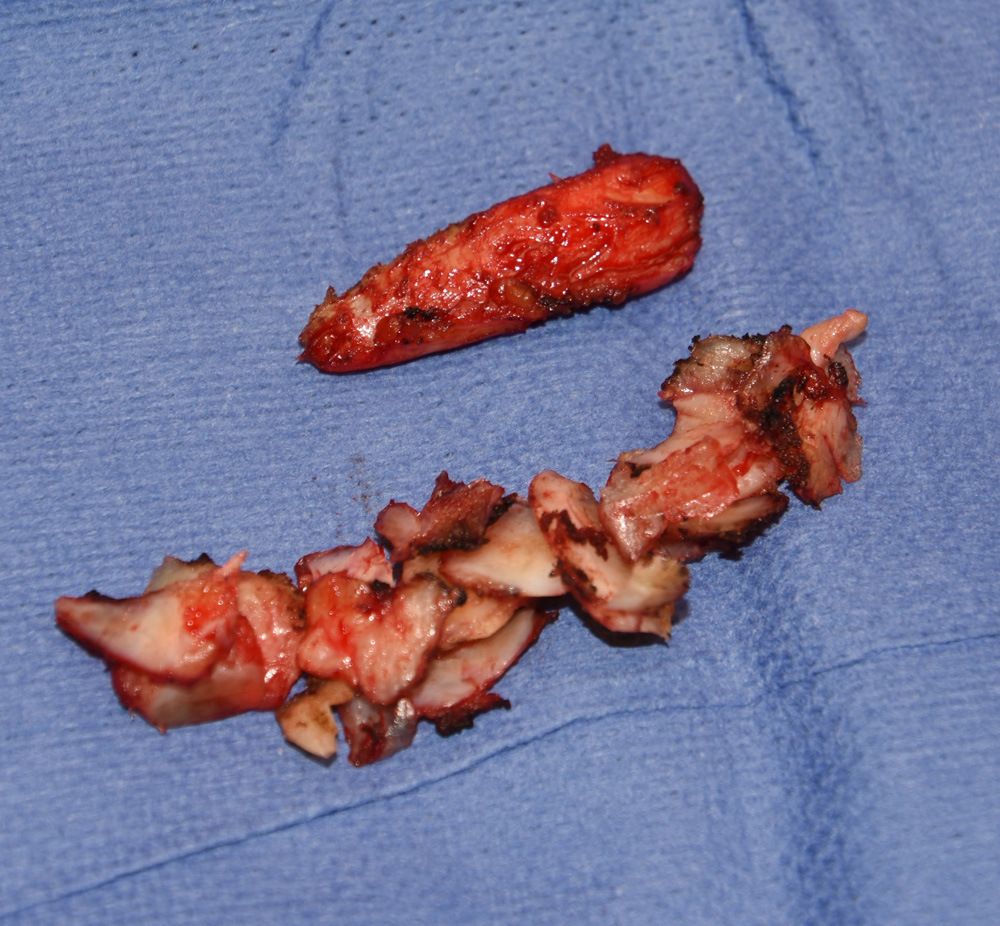 Shaving is a very effective form of rib removal/reduction that is only useful in the subcostal ribcage because of its cartulaginous composition. With enough shaving as much rib can be removed as if it was removed as a whole piece. It has the benefit of creating a smoother contour than en bloc rib resection and helps avoid direction of the back side of the rib which requires additional tissue elevation and increased risk of intercostal nerve injury and even
Shaving is a very effective form of rib removal/reduction that is only useful in the subcostal ribcage because of its cartulaginous composition. With enough shaving as much rib can be removed as if it was removed as a whole piece. It has the benefit of creating a smoother contour than en bloc rib resection and helps avoid direction of the back side of the rib which requires additional tissue elevation and increased risk of intercostal nerve injury and even
pneumothorax.
Highlights:
1) The ribcage is prone to traumatic deformities particularly at the costochondral junctions
2) Subcostal ribcage protrusions can be reduced through a direct incisional approach.
3) Cartilage shaving of subcostal protrusions is an effective contouring technique that avoids sharp edge demarcations.
Dr. Barry Eppley
Indianapolis, Indiana