

Background: Chin reduction remains an infrequently performed and challenging procedure. It is a far ‘simpler’ aesthetic prospect to stretch out the soft tissues of a bony prominence through implants or osteotomies (chin expansion) than it is to do a bony chin reduction. While often believed that simple burring of the bone from an intraoral approach will work, and it does for horizontal bony reduction, it often creates secondary soft tissue issues.
When soft tissues are detached from the bone and the bone support simultaneously reduced, there is a high risk of a subsequent soft tissue sag. This is well chronicled in both chin and cheek reductions. While it would be great if the facial soft tissues always contracted and shrunk down around areas of reduced bone support…this is not always so.
Appreciation of soft tissue sags and redundancies serves as the basis for a submental chin reduction approach. And it also is how soft tissue problems after other chin reduction approaches are managed.
Case Study: This female was bothered by her overprojecting chin. This was present both at rest and when smiling. It was too vertically long and had slightly too much horizontal projection. Its width and current shape was acceptable.

 Under general anesthesia and through a submental incision, a 5mm vertical bony chin reduction was initially done. Then a 3mm horizontal bony chin was done. A full-thickness segment of skin, fat and muscle was removed and the soft tissues tightened around the reduced chin bone.
Under general anesthesia and through a submental incision, a 5mm vertical bony chin reduction was initially done. Then a 3mm horizontal bony chin was done. A full-thickness segment of skin, fat and muscle was removed and the soft tissues tightened around the reduced chin bone.

 The submental chin reduction technique provides direct visual access for the best 3D bony chin reduction result. It allows the opportunity to do so while staying well below the exit of the mental nerve from the sides of the bone, making the risk of lip numbness negligible. It also allows for the opportunity, and almost always a necessity, to reduce excessive soft tissue and tighten it around the chin bone.
The submental chin reduction technique provides direct visual access for the best 3D bony chin reduction result. It allows the opportunity to do so while staying well below the exit of the mental nerve from the sides of the bone, making the risk of lip numbness negligible. It also allows for the opportunity, and almost always a necessity, to reduce excessive soft tissue and tighten it around the chin bone.
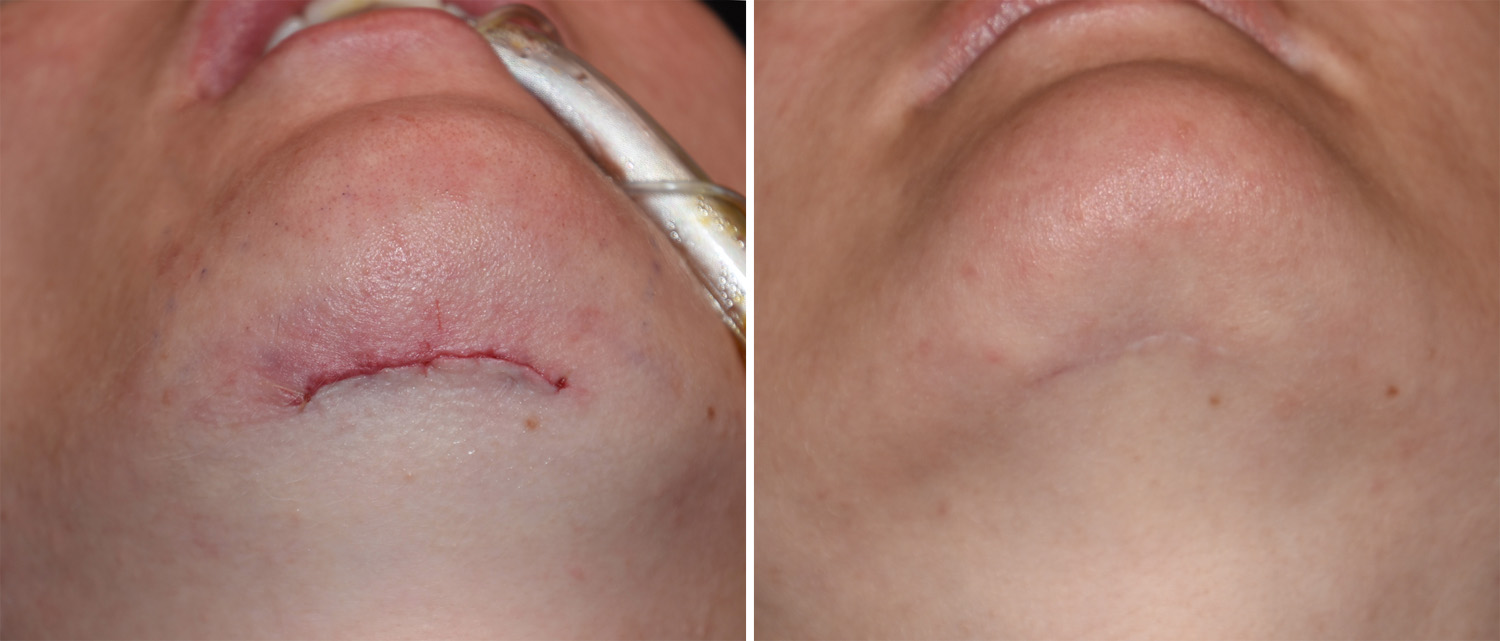 But the submental chin reduction does place a scar under the chin and this is always an aesthetic concern. These scars typically heal well and the incisional appearance is almost never a concern. There may be a need for a secondary submental soft tissue revision as the desire to limit the length of the scar must be balanced against how much soft tissue to remove. during the tuck part of the procedure. This means that occasionally there may be some soft tissue redundancies (dog ears) that appear at the end of the incision only seen after complete healing.
But the submental chin reduction does place a scar under the chin and this is always an aesthetic concern. These scars typically heal well and the incisional appearance is almost never a concern. There may be a need for a secondary submental soft tissue revision as the desire to limit the length of the scar must be balanced against how much soft tissue to remove. during the tuck part of the procedure. This means that occasionally there may be some soft tissue redundancies (dog ears) that appear at the end of the incision only seen after complete healing.
Highlights:
1) A 3D chin reduction is often done best by a submental approach.
2) With bone reduction often comes the need for soft tissue reduction as well to prevent soft tissue pad sagging or excess.
3) The submental chin reduction incision heals well but soft tissue redundancies at their ends may need to be revised secondarily.
Dr. Barry Eppley
Indianapolis, Indiana