

Background: A more well-defined jawline has become an aesthetic goal for many men and women today. While twenty years ago it was all about the amount of horizontal chin projection of the front of the jawline (and that is still true today), the back part of the jaw (jaw angles) is also recognized now as significant as well. A more complete approach to jawline aesthetics considers the entire length of the bone from front to back if a better total jawline appearance is to be obtained.
It would be no surprise that if a chin is deficient, the jaw angles may be as well since the development of the lower jaw (mandible) is the same throughout its length. A short chin will often have a high jaw angle as a result of how the bone naturally develops. The position of the lower end of the jaw angle and the chin creates the mandibular plane angle which is steep in many underdeveloped lower jaws.
 Historically, jaw angle augmentation was viewed as a width increase of the jaw angles. While a lateral width increase may enhance the appearance of the jaw angles, this dimensional change is rarely adequate for most jawline enhancement needs. A vertical increase is just, if not more, significant than any amount of jaw angle widening. It becomes important to lower the mandibular plane angle, or rotate the jaw down in the back, to obtain a more aesthetic jaw angle change to improve the overall facial appearance.
Historically, jaw angle augmentation was viewed as a width increase of the jaw angles. While a lateral width increase may enhance the appearance of the jaw angles, this dimensional change is rarely adequate for most jawline enhancement needs. A vertical increase is just, if not more, significant than any amount of jaw angle widening. It becomes important to lower the mandibular plane angle, or rotate the jaw down in the back, to obtain a more aesthetic jaw angle change to improve the overall facial appearance.
Case Study: This 48 year-old male wanted to improve the definition/strength of his lower jawline. While he was happy with his chin projection/shape, he felt the back part of his lower jaw was deficient. He wanted stronger jaw angles but also did not want them too big or prominent. He wanted them to fit well into the overall structure of his face.
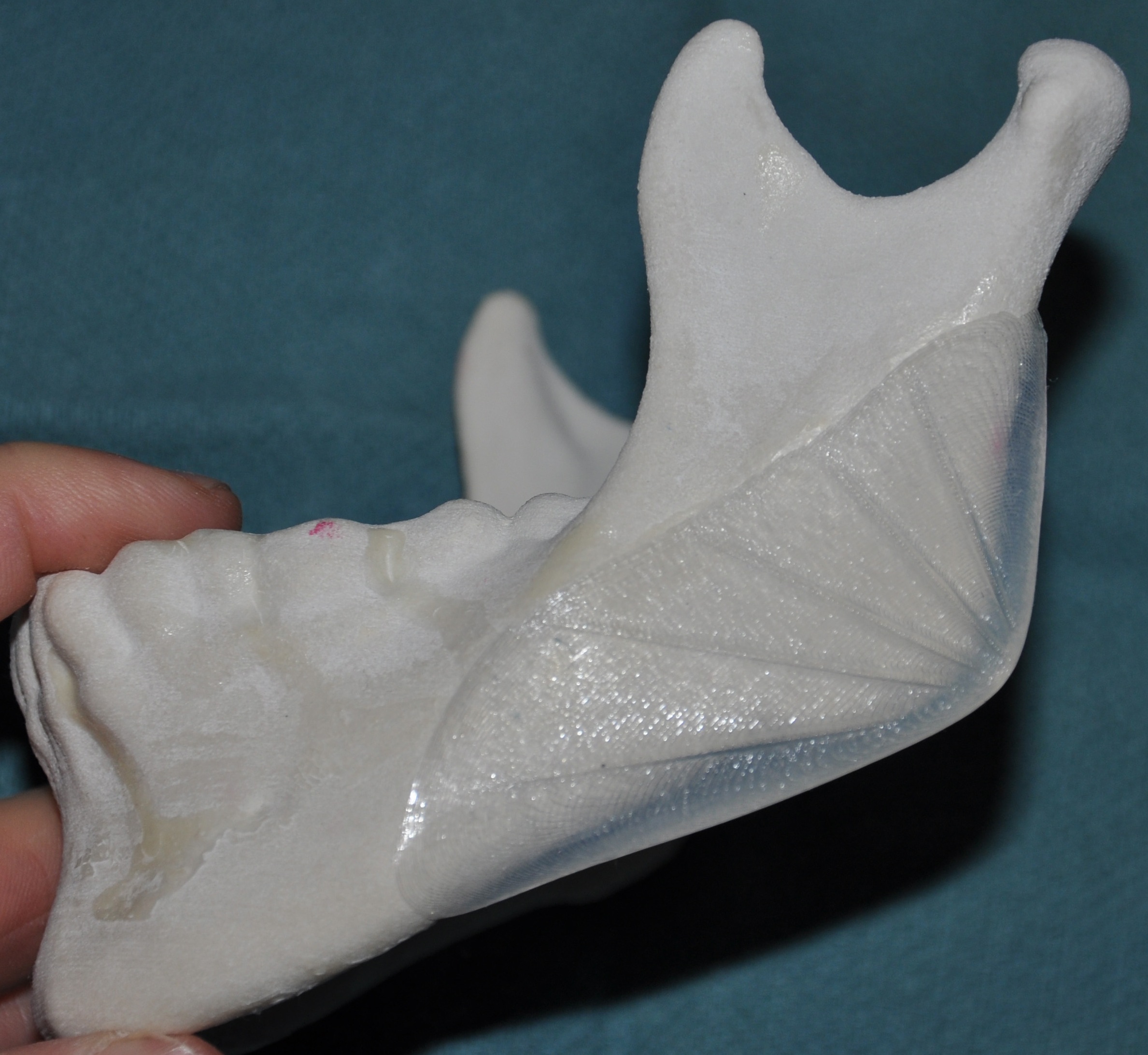
 Under general anesthesia, an intraoral approach using posterior vestibular incisions allowed access to the bony jaw angle areas. Subperiosteal dissection gently lifted off the attachments along the lower border of the mandible back around the jaw angle area onto the posterior border of the ramus. Vertical lengthening jaw angle implants (7mm vertical and 5mms width) were placed, positioning them with the lower half of the implant below the bone. There were secured into position with a single 1.5 x 7mm screw placed intraorally. After antibiotic irrigation, a two-layer closure was done (muscle and mucosa) with resorbable sutures.
Under general anesthesia, an intraoral approach using posterior vestibular incisions allowed access to the bony jaw angle areas. Subperiosteal dissection gently lifted off the attachments along the lower border of the mandible back around the jaw angle area onto the posterior border of the ramus. Vertical lengthening jaw angle implants (7mm vertical and 5mms width) were placed, positioning them with the lower half of the implant below the bone. There were secured into position with a single 1.5 x 7mm screw placed intraorally. After antibiotic irrigation, a two-layer closure was done (muscle and mucosa) with resorbable sutures.
 While there will be some swelling of the jaw angles, half of it is gone by ten days and almost all of it by three weeks after surgery. A 7mm vertical jaw angle lengthening does not sound like much, but can create a noticeable change in the jawline that does not have an overly high jaw angle position.
While there will be some swelling of the jaw angles, half of it is gone by ten days and almost all of it by three weeks after surgery. A 7mm vertical jaw angle lengthening does not sound like much, but can create a noticeable change in the jawline that does not have an overly high jaw angle position.
Case Highlights:
1) A posterior jaw angle deficiency more often than not involves a vertical deficiency as much as any horizontal deficiency. (the high jaw angle)
2) Vertical lengthening jaw angle implants provide a downward and outer rotation to the appearance of the back part of the jaw.
3) Vertical lengthening jaw angle implants require careful pocket dissection to avoid avulsion of the pteryomasseteric sling anatomy and retraction of the masseter muscle superiorly.
Dr. Barry Eppley
Indianapolis, Indiana