

Background: A webbed neck, medically known as pterygium colli deformity, is a well known but rare congenital neck condition. Skin folds are present along the sides of the neck from the back of the head behind the ears down to the shoulders. The hairline often follows the skin folds in their upper part. It is most commonly seen in Turner’s syndrome but occurs on congenital syndromes as well. The skin folds occur in varying presentations but can be quite pronounced in many cases.
The surgical correction of the webbed neck has evolved from original descriptions of z-plasties done directly along the skin folds. While successfully breaking up the skin folds, such a direct approach leaves unsightly scars that are rarely worth the trade-off.
The posterior approach to the webbed neck is the preferred technique today. This involves removing tissue from the midline of the posterior neck and wide skin undemining out to the skin folds. Closing the posterior neck defect then pulls the skin folds inward. (more posteriorly) A variety of posterior neck excisional patterns have been described from butterfly, M and Z-plasty patterns. While providing definite improvement in the appearance of the skin folds and keeping the scar fairly hidden (with long hair), partial relapse is common with the secondary skin relaxation.
Case Study: This 35 year-old Asian female had a congenital webbed neck from birth. She did not have Turner’s or any other known congenital condition. Her necks webs would be described as mild to moderate. She was teased a lot for her neck webs when she was growing up. Prior to surgery, she shaved the lower portion of her occipital hairline to aid the subsequent surgery.
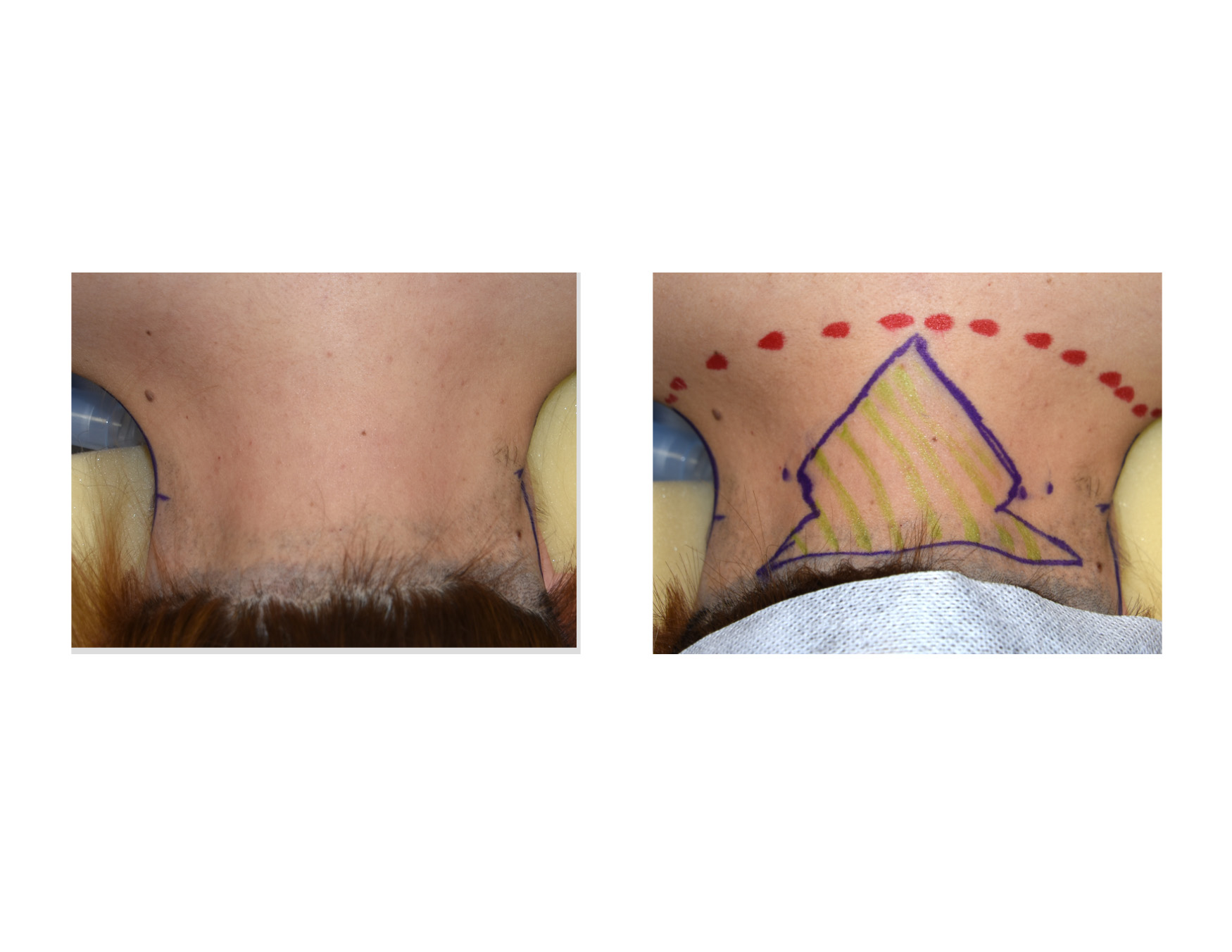 Under general anesthesia, the posterior neck was marked with red dots to mark the most tolerated lower extent of the tissue excision and midline closure and a modified T-shaped excisional pattern. The neck webs were vertically marked.
Under general anesthesia, the posterior neck was marked with red dots to mark the most tolerated lower extent of the tissue excision and midline closure and a modified T-shaped excisional pattern. The neck webs were vertically marked.
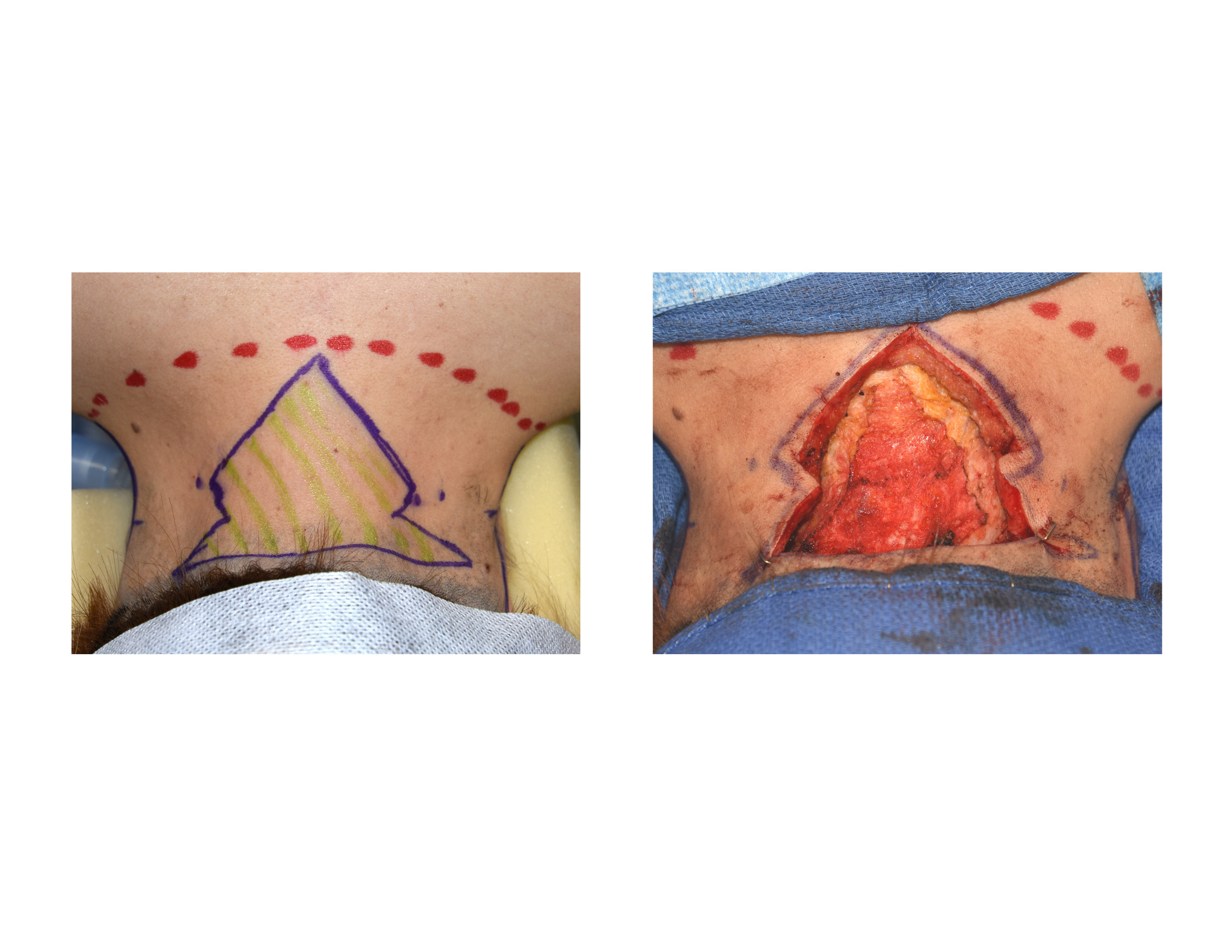
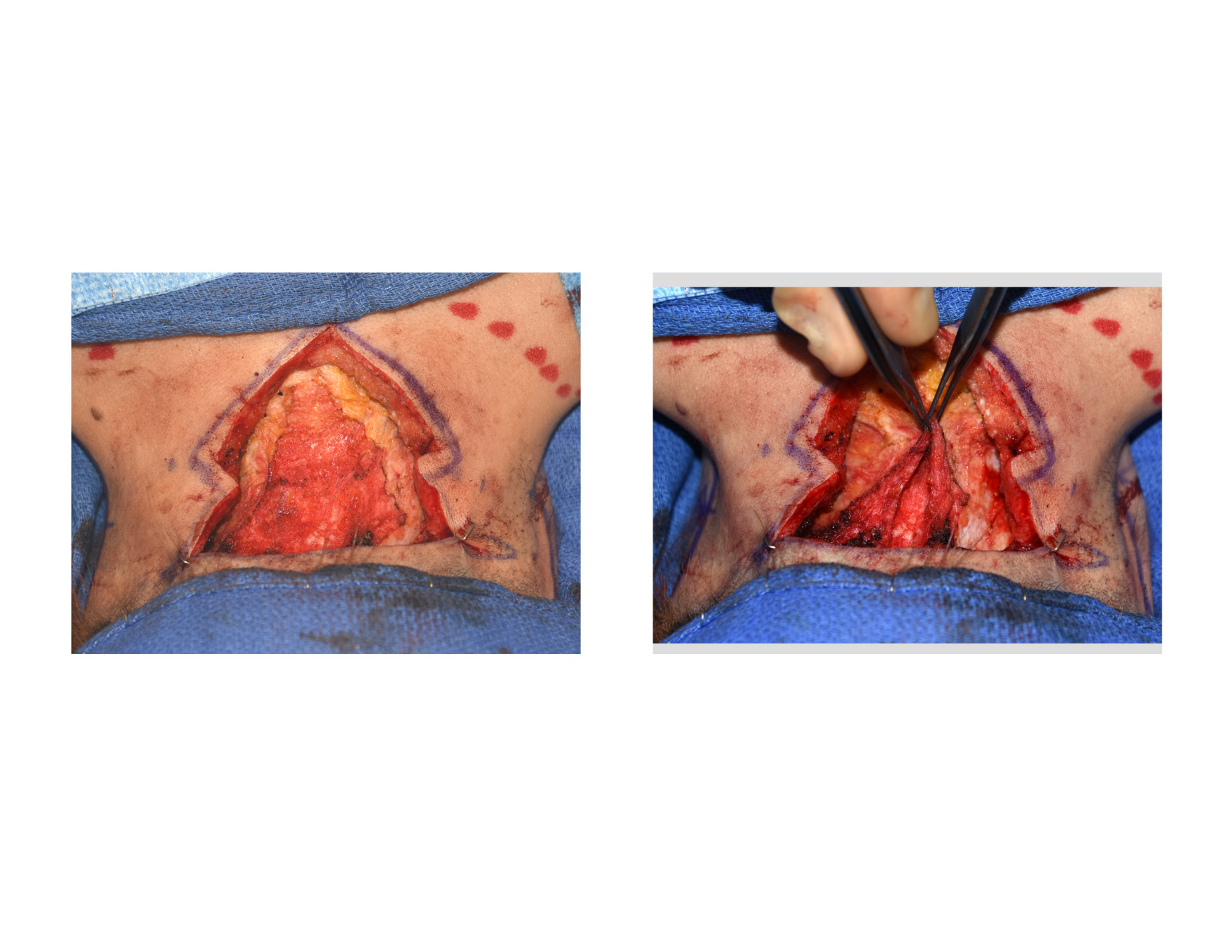 The posterior neck skin and fat was excised down to fascia. The skin edges were widely undermined out to the skin folds. The fascia edges could be grasped and mobilized considerably to the midline.
The posterior neck skin and fat was excised down to fascia. The skin edges were widely undermined out to the skin folds. The fascia edges could be grasped and mobilized considerably to the midline.
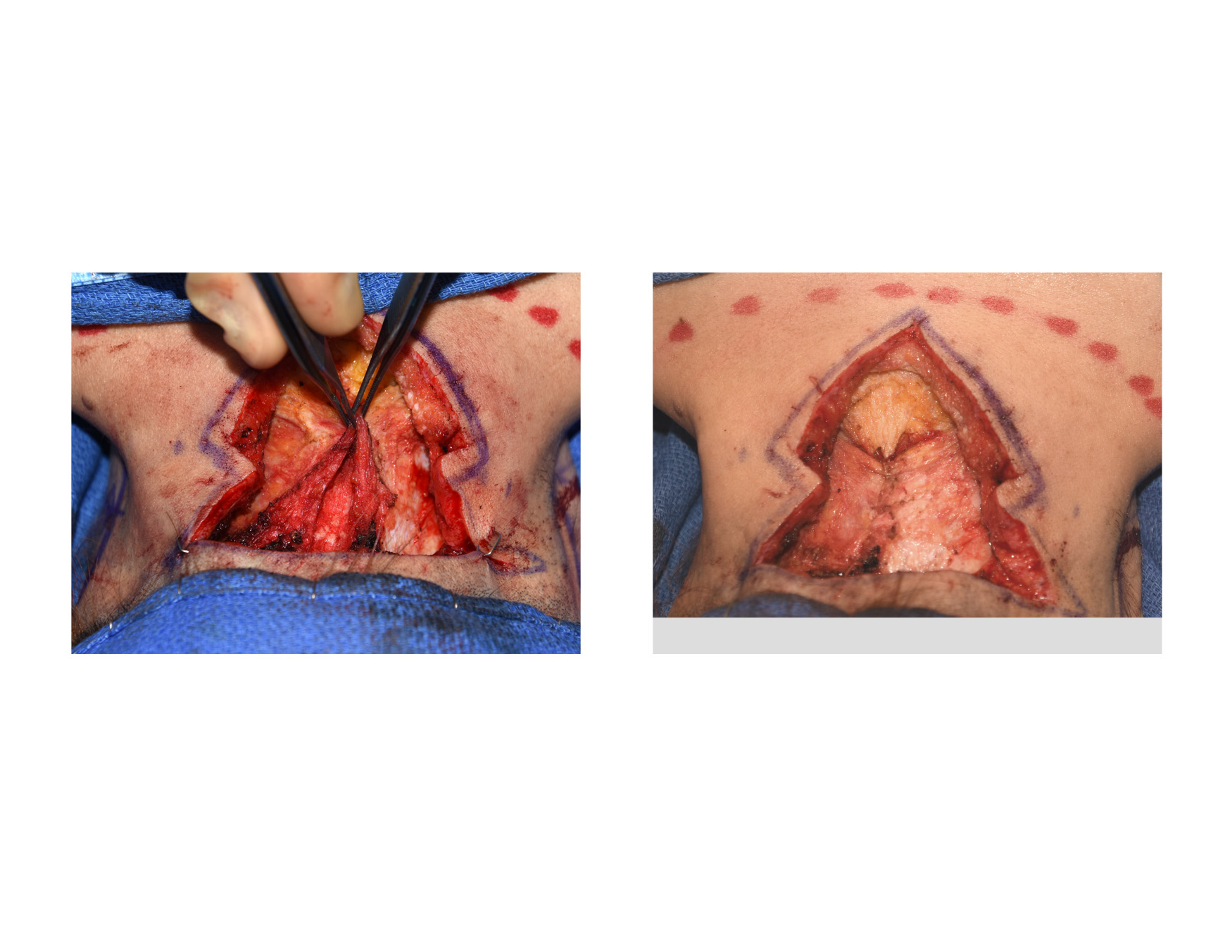 The posterior neck fascia was plicated in the midline with large resorbable sutures. This could be seen to bring in the skin folds at the side of the neck significantly.
The posterior neck fascia was plicated in the midline with large resorbable sutures. This could be seen to bring in the skin folds at the side of the neck significantly.
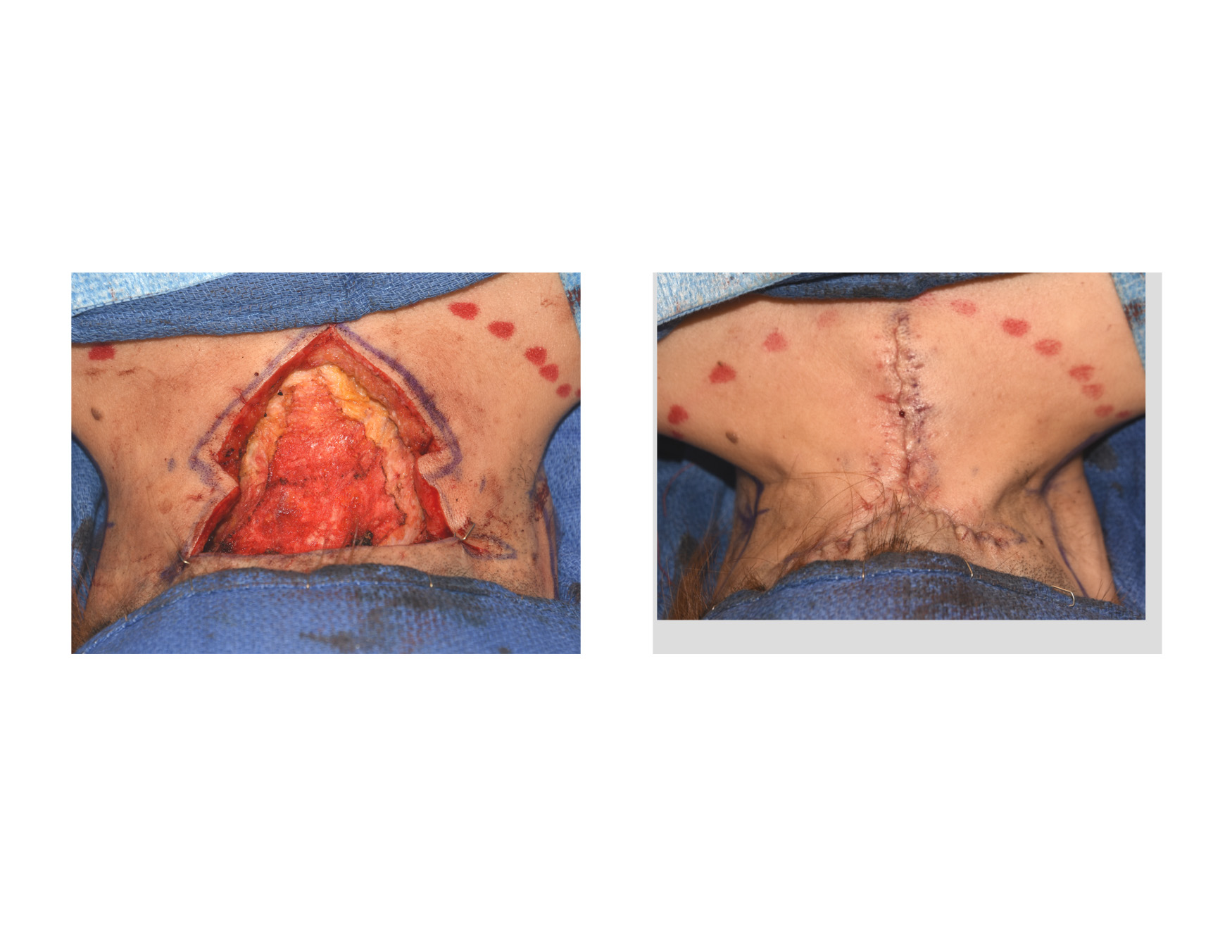 The skin edges were then brought in to the midline and closed in a T-shaped pattern. Prior to the skin closure, multiple quilting sutures were placed from the skin down to the fascia to both eliminate deep space as well as take tension off the skin closure suture line. Marcaine injections were done along the fascia as well as the greater and lesser occipital nerves to manage immediate postoperative discomfort. The posterior neck incisions were covered only with with tapes.
The skin edges were then brought in to the midline and closed in a T-shaped pattern. Prior to the skin closure, multiple quilting sutures were placed from the skin down to the fascia to both eliminate deep space as well as take tension off the skin closure suture line. Marcaine injections were done along the fascia as well as the greater and lesser occipital nerves to manage immediate postoperative discomfort. The posterior neck incisions were covered only with with tapes.
 The skin folds were completely eliminated with this webbed neck surgery technique. The neck was changed from wide neck ‘wings’ to an hourglass neck appearance.
The skin folds were completely eliminated with this webbed neck surgery technique. The neck was changed from wide neck ‘wings’ to an hourglass neck appearance.
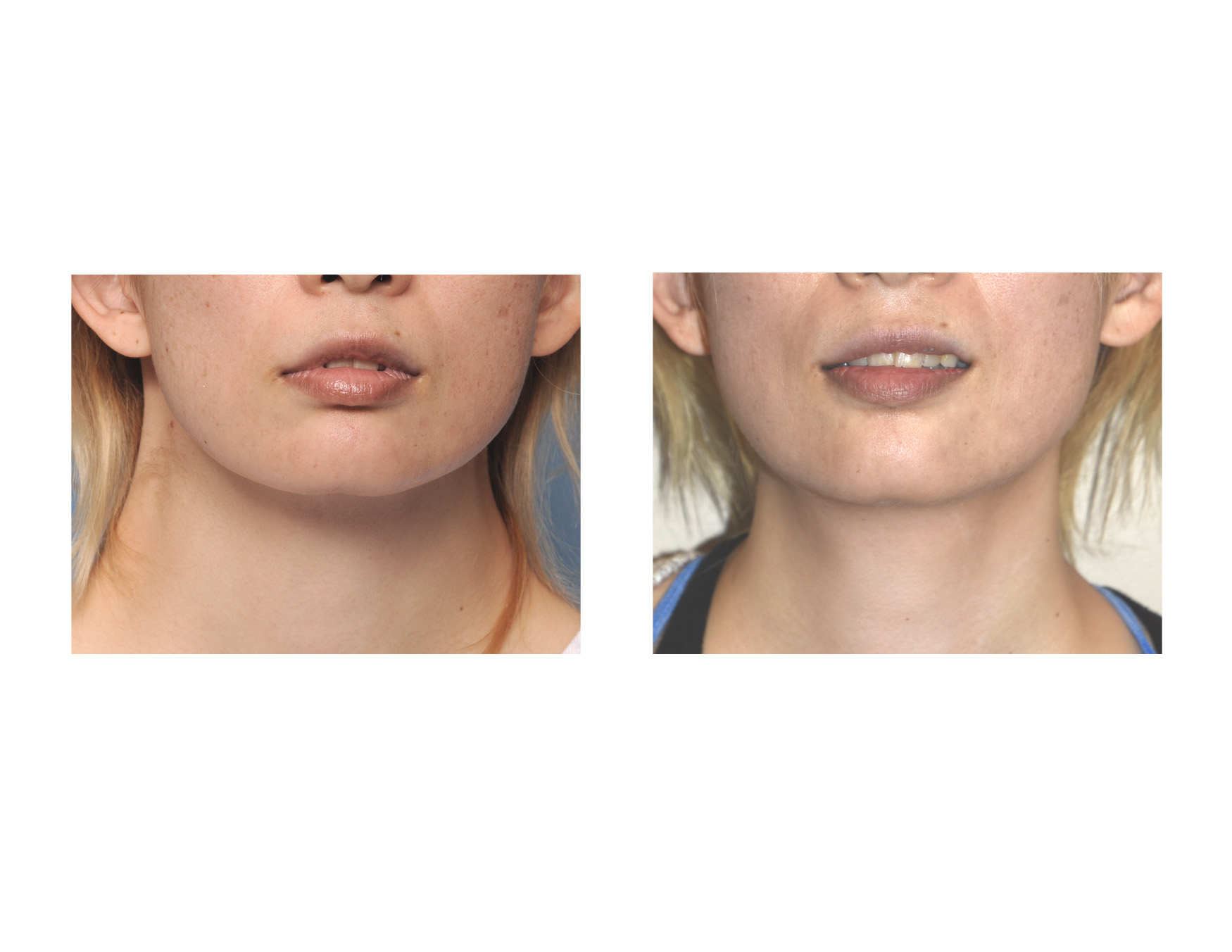
 When seen the next day after surgery before returning home, her webbed neck condition was completely eliminated. The combination of posterior neck tissue excision and midline fascial plication creates an improved and sustained result in webbed neck surgery.
When seen the next day after surgery before returning home, her webbed neck condition was completely eliminated. The combination of posterior neck tissue excision and midline fascial plication creates an improved and sustained result in webbed neck surgery.
Highlights:
1) Webbed neck correction requires a posterior neck approach with tissue excision and midline closure to prevent visible scars on the sides of the neck.
2) Midline fascial plication is critical to bring in the sides of the neck (webs) and relieve tension on the posterior midline neck closure.
3) This form of webbed neck surgery uses the same principles as midline platysmal plication in facelift or direct anterior necklift surgery.
Dr. Barry Eppley
Indianapolis, Indiana