

ackground: The ear is made up of a complex array of ridges and depressions in a very small anatomic area. The dominant features of the ear is the external helical ridge with an internal antihelical ridge, both of which surround the bowl of the ear (concha) which surrounds the ear canal. Normally the outer helix sits just above the antihelix with an ear protrusion from the side of the head no greater than about 25 degrees or less than 2 cms from the helix to the mastoid.. When the antihelix is absent (underdeveloped antihelical fold) or the concha is very large, the ears will become protrusive or stick out.
 While medical evidence now indicates that our ears do continue to slowly grow throughout life, their greatest growth occurs in the first ten years after birth. It is often stated that 80% to 85% percent of ear growth occurs by age 6. This has been the reason that corrective otoplasty surgery has not been historically recommended to be done before that age…to avoid damaging the growing ear.
While medical evidence now indicates that our ears do continue to slowly grow throughout life, their greatest growth occurs in the first ten years after birth. It is often stated that 80% to 85% percent of ear growth occurs by age 6. This has been the reason that corrective otoplasty surgery has not been historically recommended to be done before that age…to avoid damaging the growing ear.
But as children enter school environments earlier then ever before, some parents are interested in having protruding ears corrected before six years of age. Since otoplasty surgery is not an excisional or destructive procedure, such intervention is deemed as safe and does not disturb subsequent ear growth. Some plastic surgery studies have shown that otoplasty can be safely performed as young as two years old.
Case Study: This 4 year-old male child was seen with a parental request to have ears corrected. He had large protruding ears with the complete absence of antihelical folds and large conchal bowls. The felt it would be best to correct his protruding ears now as opposed to waiting until he was older.
Under general anesthesia, he underwent an otoplasty correction using two different suture techniques. The antihelical folds were created using multiple horizontal mattress sutures of 4-0 monocryl. The concha was set back using a single 4-0 monocryl suture between the conchal cartilage and the mastoid fascia. Only a thin strip of skin was removed from the back of the ear for the incisional access.
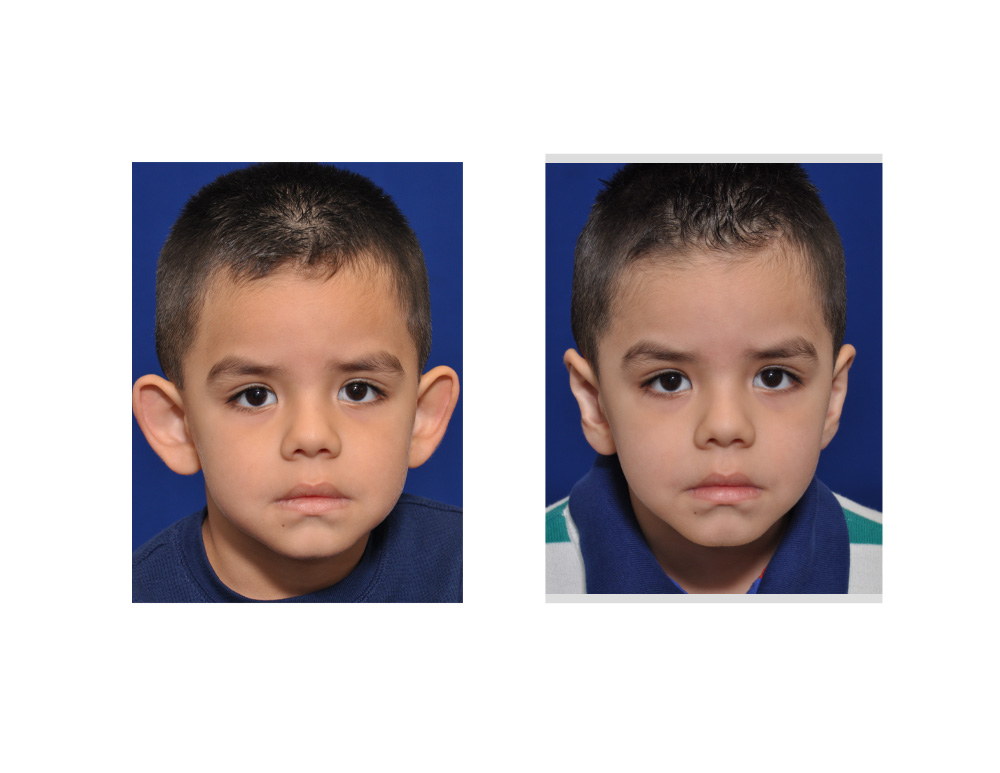
 His otoplasty results shows a tremendous improvement in the shape of his ears in both the front and back views. He had no significant pain after surgery although his ears will remain sensitive for a few months after surgery. No ear growth problems would be expected to occur as the ear cartilage was simply folded and sutured. In young children it is best to use dissolveable sutures as opposed to permanent ones to avoid any risk of long-term suture reactions/extrusions.
His otoplasty results shows a tremendous improvement in the shape of his ears in both the front and back views. He had no significant pain after surgery although his ears will remain sensitive for a few months after surgery. No ear growth problems would be expected to occur as the ear cartilage was simply folded and sutured. In young children it is best to use dissolveable sutures as opposed to permanent ones to avoid any risk of long-term suture reactions/extrusions.
Case Highlights:
1) Otoplasty is an effective procedure for reshaping the protruding ear.
2) Otoplasty can be done at a very early age using suture techniques without harming future ear growth.
3) Dissolveable or permanent sutures can be used in early age otoplasties.
Dr. Barry Eppley
Indianapolis, Indiana