

The jaw angle is a critical element of lower facial aesthetics, particularly in men. While perceptions of an attractive jawline vary by individual preference, most people instinctively recognize a strong, well-defined jaw angle when they see it. Beyond subjective impressions, however, the jaw angle can be quantified through several established cephalometric measurements, which have been used for decades to analyze and guide treatment of facial form.
Key Measurements of Jaw Angle Aesthetics
There are three commonly used measurements to assess the jaw angle, each offering a different dimensional perspective:
-
 Gonial Angle: This is the direct angle formed by the intersection of the posterior and inferior borders of the mandible. Attractive gonial angles typically fall between 115° and 130°. Angles below 110° can appear overly strong or prominent (too low), while those above 130°–140° often look indistinct or weak (too high).
Gonial Angle: This is the direct angle formed by the intersection of the posterior and inferior borders of the mandible. Attractive gonial angles typically fall between 115° and 130°. Angles below 110° can appear overly strong or prominent (too low), while those above 130°–140° often look indistinct or weak (too high). -
Mandibular Plane Angle: This measures the slope of the jawline relative to the anterior skull base (either the sella-nasion or Frankfort horizontal line). The mandibular plane angle normally ranges from 25° to 30°. A higher angle blurs the distinction between face and neck and produces a narrower lower face. Conversely, a lower angle creates a clearer separation but, if excessive, can result in a boxy appearance.
-
Bizygomatic Width: This is the horizontal width across the cheekbones at the peaks of the zygomatic arches. It serves as a reference point to compare the proportions of the mid- and lower face, but it must be adjusted for differences in soft tissue thickness between the cheeks and jaw angles.
 Gonial Angle: This is the direct angle formed by the intersection of the posterior and inferior borders of the mandible. Attractive gonial angles typically fall between 115° and 130°. Angles below 110° can appear overly strong or prominent (too low), while those above 130°–140° often look indistinct or weak (too high).
Gonial Angle: This is the direct angle formed by the intersection of the posterior and inferior borders of the mandible. Attractive gonial angles typically fall between 115° and 130°. Angles below 110° can appear overly strong or prominent (too low), while those above 130°–140° often look indistinct or weak (too high).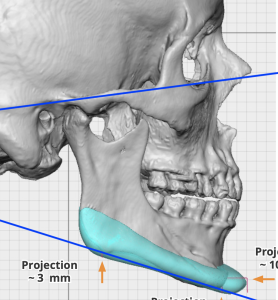 Mandibular Plane Angle: This measures the slope of the jawline relative to the anterior skull base (either the sella-nasion or Frankfort horizontal line). The mandibular plane angle normally ranges from 25° to 30°. A higher angle blurs the distinction between face and neck and produces a narrower lower face. Conversely, a lower angle creates a clearer separation but, if excessive, can result in a boxy appearance.
Mandibular Plane Angle: This measures the slope of the jawline relative to the anterior skull base (either the sella-nasion or Frankfort horizontal line). The mandibular plane angle normally ranges from 25° to 30°. A higher angle blurs the distinction between face and neck and produces a narrower lower face. Conversely, a lower angle creates a clearer separation but, if excessive, can result in a boxy appearance.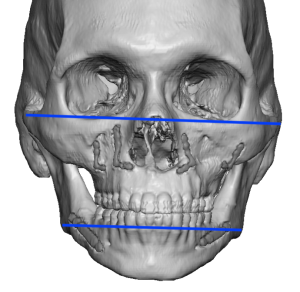 Bizygomatic Width: This is the horizontal width across the cheekbones at the peaks of the zygomatic arches. It serves as a reference point to compare the proportions of the mid- and lower face, but it must be adjusted for differences in soft tissue thickness between the cheeks and jaw angles.
Bizygomatic Width: This is the horizontal width across the cheekbones at the peaks of the zygomatic arches. It serves as a reference point to compare the proportions of the mid- and lower face, but it must be adjusted for differences in soft tissue thickness between the cheeks and jaw angles.Application to Custom Jawline Implant Design
While these angular measurements are invaluable in orthodontics, cephalometry, and jaw osteotomies, they also have relevance in designing custom jawline implants. However, their application must always consider the patient’s overall facial structure, soft tissue characteristics, and aesthetic goals.
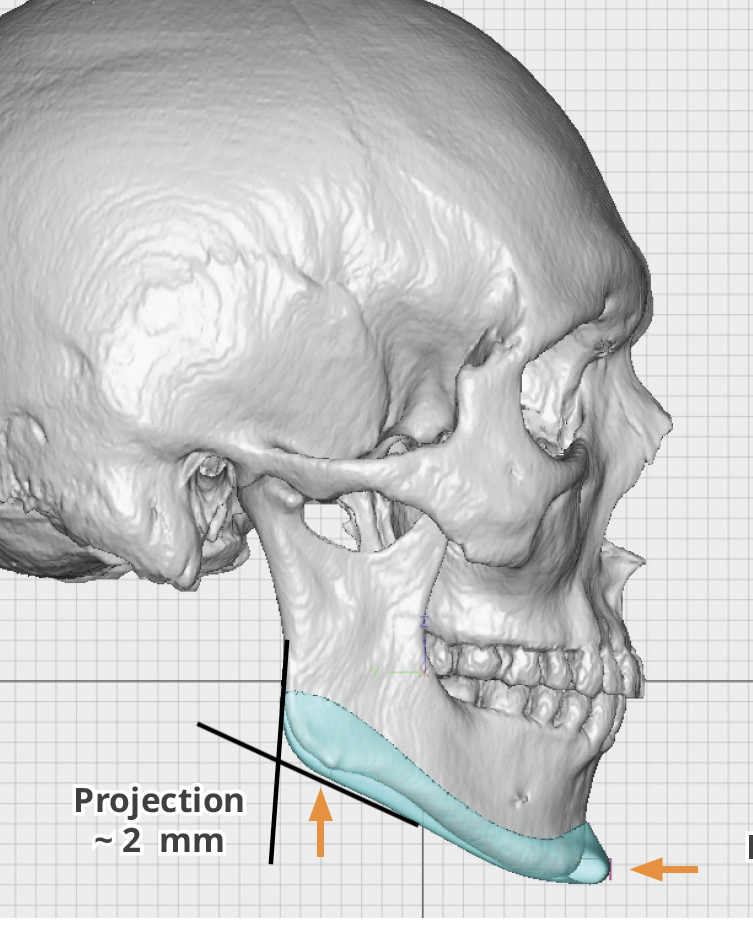
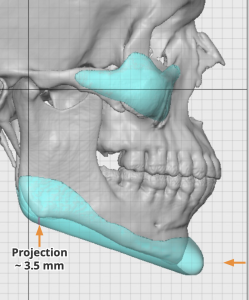 Many patients seeking jawline augmentation present with normal gonial and mandibular plane angles but lack adequate shape or width at the jaw angles. In such cases, vertical changes may not be necessary, and the design focuses on creating a more defined contour. Slight vertical jaw angle lengthening may be done for an enhanced jaw angle shape but this would be fairly small.
Many patients seeking jawline augmentation present with normal gonial and mandibular plane angles but lack adequate shape or width at the jaw angles. In such cases, vertical changes may not be necessary, and the design focuses on creating a more defined contour. Slight vertical jaw angle lengthening may be done for an enhanced jaw angle shape but this would be fairly small.
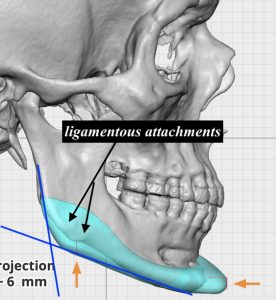
One common pitfall is attempting to “square out” the gonial angle excessively in the implant design. While the gonial angle may appear sharp on radiographs, creating a truly square corner increases the risk of masseteric muscle dehiscence and implant visibility (show). This risk is particularly pronounced when the implant extends the bony angle and requires the surrounding ligaments to stretch in a non-anatomic direction.
When Vertical Lengthening Is Indicated
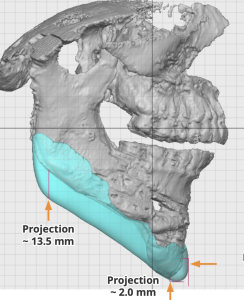
 The mandibular plane angle can guide decisions about vertical lengthening of the jaw angle. A high mandibular plane angle combined with a high gonial angle almost always benefits aesthetically from vertical lengthening to lower the jaw angles.
The mandibular plane angle can guide decisions about vertical lengthening of the jaw angle. A high mandibular plane angle combined with a high gonial angle almost always benefits aesthetically from vertical lengthening to lower the jaw angles.
Other scenarios where vertical lengthening may be advantageous include:
-
Following a previous vertical-lengthening bony genioplasty.
-
To create a more linear jawline when a prominent antegonial notch is present.
-
To lengthen a vertically short face.
 Following a previous vertical-lengthening bony genioplasty.
Following a previous vertical-lengthening bony genioplasty.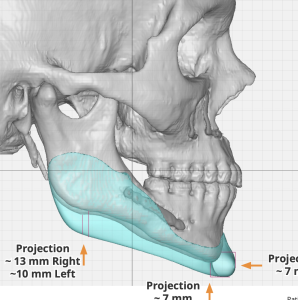 To lengthen a vertically short face.
To lengthen a vertically short face.Even in patients with normal angular values, a modest degree of vertical lengthening can improve the visibility of the augmented shape and help achieve a more linear jawline.
Balancing Width in Implant Design
When considering implant width, the primary objective is to establish an appropriate jaw angle (bigonial) width relative to the midface (bizygomatic) width. While some believe these two should be equal, this overlooks the fact that soft tissues over the zygomatic arches are significantly thinner than over the jaw angles.
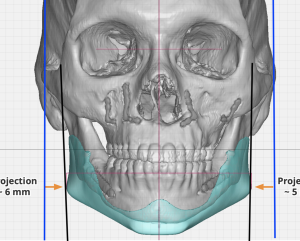 The masseter muscle alone can add 15 mm or more to the soft tissue thickness at the jaw angles, making the lower face appear wider. Therefore, the bigonial width should always remain slightly narrower than the bizygomatic width. My guideline is to keep the bigonial width at least 5 mm inside the zygomatic arch width to avoid creating a boxy or inverted facial triangle.
The masseter muscle alone can add 15 mm or more to the soft tissue thickness at the jaw angles, making the lower face appear wider. Therefore, the bigonial width should always remain slightly narrower than the bizygomatic width. My guideline is to keep the bigonial width at least 5 mm inside the zygomatic arch width to avoid creating a boxy or inverted facial triangle.
The Role of Bony Landmarks: Guidelines, Not Absolutes
Bony landmarks and cephalometric measurements provide reliable, predictable results in skeletal surgery. However, when designing implants — where the aesthetic outcome depends on soft tissue response — these landmarks serve only as general guidelines. Soft tissue variability among patients introduces unpredictability that skeletal measurements alone cannot address.
Thus, while these measurements are indispensable starting points, they should always be applied judiciously, factoring in each patient’s unique soft tissue anatomy and desired aesthetic result.
Barry Eppley, MD, DMD
World-Renowned Plastic Surgeon