

Cheekbone reduction is the only facial reshaping procedure in which one reduce the size or width of their cheekbones. It is essentially an inward repositioning of the zygomatic arch which acts like a bridge over the temporalis muscle as it descends to attach to the coronoid process of the lower jaw. The arch bone has an outward convex shape which is what gives the cheek its width to the face. The convex shape of the bone can not be changed but its anterior and posterior attachments can be released and moved inward, thus being the basis for cheekbone reduction osteotomies.
Performing the posterior arch osteotomy can only be done one way with an oblique or angled bone cut approached through a small incision at the back edge of the sideburn hair. This allows the posterior thin arch bone to be moved inward where it can be secured with a small stair-step plate. The anterior zygomatic osteotomy, which is approached through the mouth, can be done with varying osteotomy pattern designs. The bone is thicker and permits different patterns of the bone cut.
Most simplistically a straight line cut can be made at the junction of the posterior zygoma and the front end of the zygomatic arch. While this bone cut goes through the least amount of bone, placing a bone cut in this location makes it hard to apply plate fixation to the arch segment with poor angulation for screw placement and a small bone segment to engage. It also does not place the bone cut far enough forward to bring in the some the anterior cheek bone width.
 More commonly an obliquely oriented straight line cut is made through the main body of the zygoma at more of a sagittal angle. A 3 to 4mm wedge of bone is removed and teh segments plated together. This more anterior approach to the osteotomy allows less soft tissue to be stripped of their attachments for exposure. This may go a long way to avoiding postoperative cheek sagging.
More commonly an obliquely oriented straight line cut is made through the main body of the zygoma at more of a sagittal angle. A 3 to 4mm wedge of bone is removed and teh segments plated together. This more anterior approach to the osteotomy allows less soft tissue to be stripped of their attachments for exposure. This may go a long way to avoiding postoperative cheek sagging.
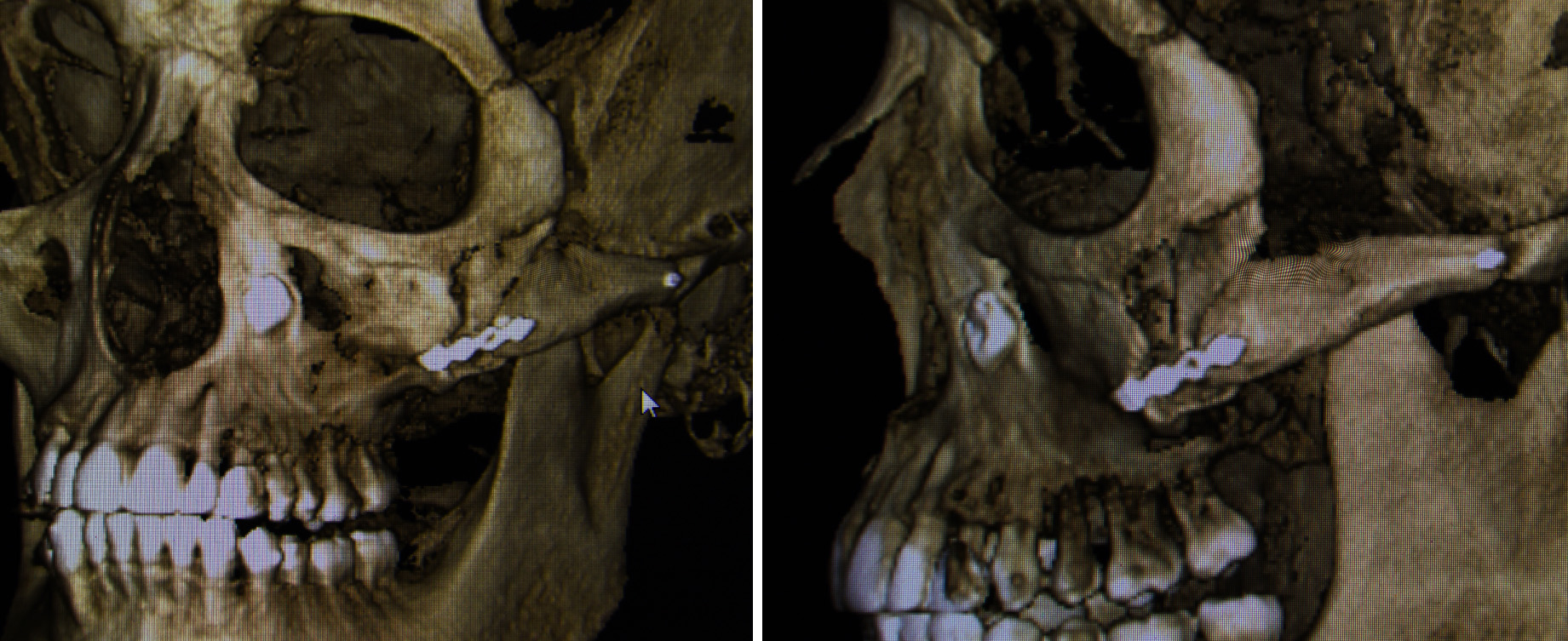 Another popular anterior cheek osteotomy approach is the L, combining a vertical bone cut with an oblique one running through the superior zygoma. This technique has the advantage of allowing a smaller segment of bone to be removed while also maximizing the amount of bone contact for plate fixation and healing. There is also the variation of cresting a double osteotomy line which allows the bone to be reshaped and moved inward without having to remove any actual bone. Plate fixation makes it possible for this more complex anterior zygomatic osteotomy to be successfully performed.
Another popular anterior cheek osteotomy approach is the L, combining a vertical bone cut with an oblique one running through the superior zygoma. This technique has the advantage of allowing a smaller segment of bone to be removed while also maximizing the amount of bone contact for plate fixation and healing. There is also the variation of cresting a double osteotomy line which allows the bone to be reshaped and moved inward without having to remove any actual bone. Plate fixation makes it possible for this more complex anterior zygomatic osteotomy to be successfully performed.
Dr. Barry Eppley
Indianapolis, Indiana