

The use of a chin implant for an increase in lower facial projection is often combined with other procedures (e.g., rhinoplasty) as well as done as an isolated chin augmentation. It has a long history of use in aesthetic facial surgery dating back over fifty years and nearly every available biomaterial has been tried as some form of a chin implant. But the use of silicone chin implants today constitutes the majority of chin augmentation devices used.
One phenomenon of placing a silicone chin implant (it also occurs with other biomaterials as well) is that of ‘chin implant erosion’. This is an erroneous term that implies that a chin implant is actively eating into or destroying the chin bone underneath it. (aka an active inflammatory process occurring as a a result of a bone reaction in response to a leaking of silicone molecules from the implant) That perception and propagated term is far from what actually occurs.
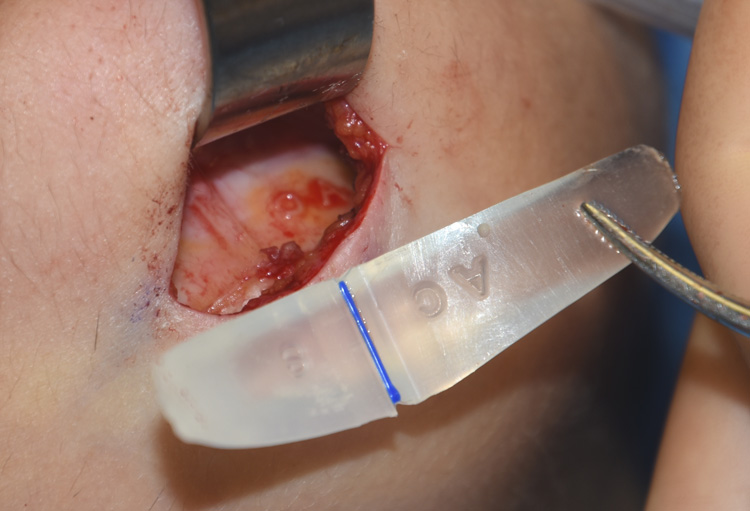 The chin is a unique facial area for augmentation because it is a projecting bony structure with tight tissue attachments that wrap around it. Thus when an implant is placed between the chin bone and the overlying soft tissues it will exert some forces (pressure) on the underlying and overlying soft tissues. The body will relieve this pressure with passive adaptation to it. Since the chin implant can not change due to its synthetic inert structure, the surrounding tissue must. As a result, the chin implant will often (although not always) settle a millimeter or two into the bone as a form of pressure relief. This can be seen in great detail as the serial number, size indicator or any grooves or markings on the implant can be seen on the bone surface as the implant is removed.
The chin is a unique facial area for augmentation because it is a projecting bony structure with tight tissue attachments that wrap around it. Thus when an implant is placed between the chin bone and the overlying soft tissues it will exert some forces (pressure) on the underlying and overlying soft tissues. The body will relieve this pressure with passive adaptation to it. Since the chin implant can not change due to its synthetic inert structure, the surrounding tissue must. As a result, the chin implant will often (although not always) settle a millimeter or two into the bone as a form of pressure relief. This can be seen in great detail as the serial number, size indicator or any grooves or markings on the implant can be seen on the bone surface as the implant is removed.
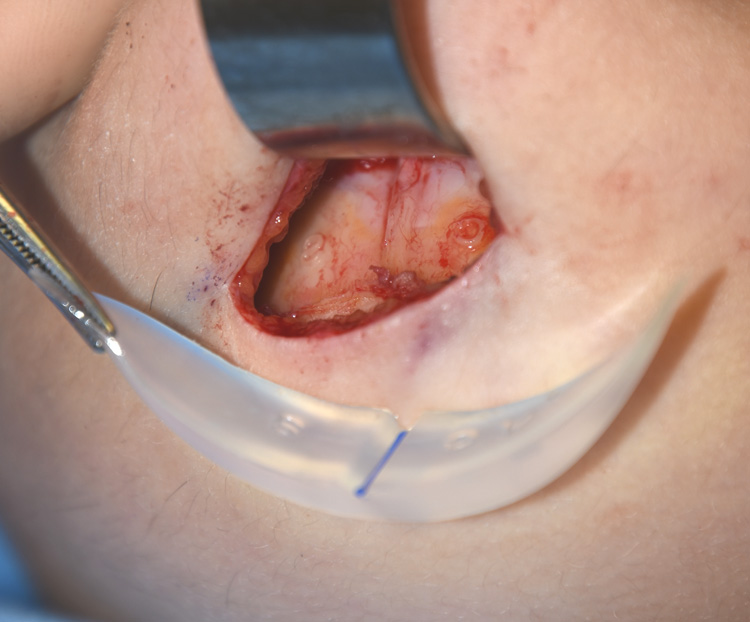 This passive bony remodeling phenomenon to a chin implant is benign and self-limiting. It has little to no impact on the external aesthetic chin augmentation result and does not affect the quality of the underlying bone. Because most chin implants are placed in the subperiosteal plane this settling will also allow some bony growth to often extend up along the sides of the implant. Such bony overgrowth can be seen clearly intraoperatively as well as on CT scans. This bony overgrowth further implies that the implant is not causing a destructive bony process.
This passive bony remodeling phenomenon to a chin implant is benign and self-limiting. It has little to no impact on the external aesthetic chin augmentation result and does not affect the quality of the underlying bone. Because most chin implants are placed in the subperiosteal plane this settling will also allow some bony growth to often extend up along the sides of the implant. Such bony overgrowth can be seen clearly intraoperatively as well as on CT scans. This bony overgrowth further implies that the implant is not causing a destructive bony process.
There are very rare cases where chin implant settling has placed the mandibular incisor tooth roots at risk or has caused some dental sensitivity. This is a direct result of a chin implant being placed far too high over the much thinner cortical bone near the tooth roots. As a result, passive implant settling may occur deeper into the bone and appear very close radiographically to the tooth roots. This is the direct result of an incorrect chin implant placement.
It is time to eliminate the term ‘chin implant erosion’ due to its biologic inaccuracy and replace it with a term that correctly identifies it with the passive bony remodeling process that it is. The better descriptor would be ‘chin implant imprinting’.
Dr. Barry Eppley
Indianapolis, Indiana