

Chin augmentation is a very effective procedure for those who suffer from microgenia or a weak chin. It is a procedure that is performed almost equally in both men and women. In males, it is more commonly done when they are younger usually under the age of 40.
It is also this male age group that is the most active from an athletic standpoint, Many of these sports activities can involve contact such as basketball, martial arts and boxing. Inadvertent blunt blows to the face of significant force are not uncommon. For those who have a chin implant, does participation in these sports play the chin implant at risk?
Several years ago, I saw a patient in my Indianapolis plastic surgery practice who suffered a chin implant ‘injury’. This was a college football player who had a chin augmentation procedure done when he was 16 years old. He was hit in the chin during a tackle and had immediate swelling. When the swelling subsided weeks later, he had obvious chin asymmetry. During surgical exploration, it was discovered that the silicone implant had shifted off midline as a result of the trauma.
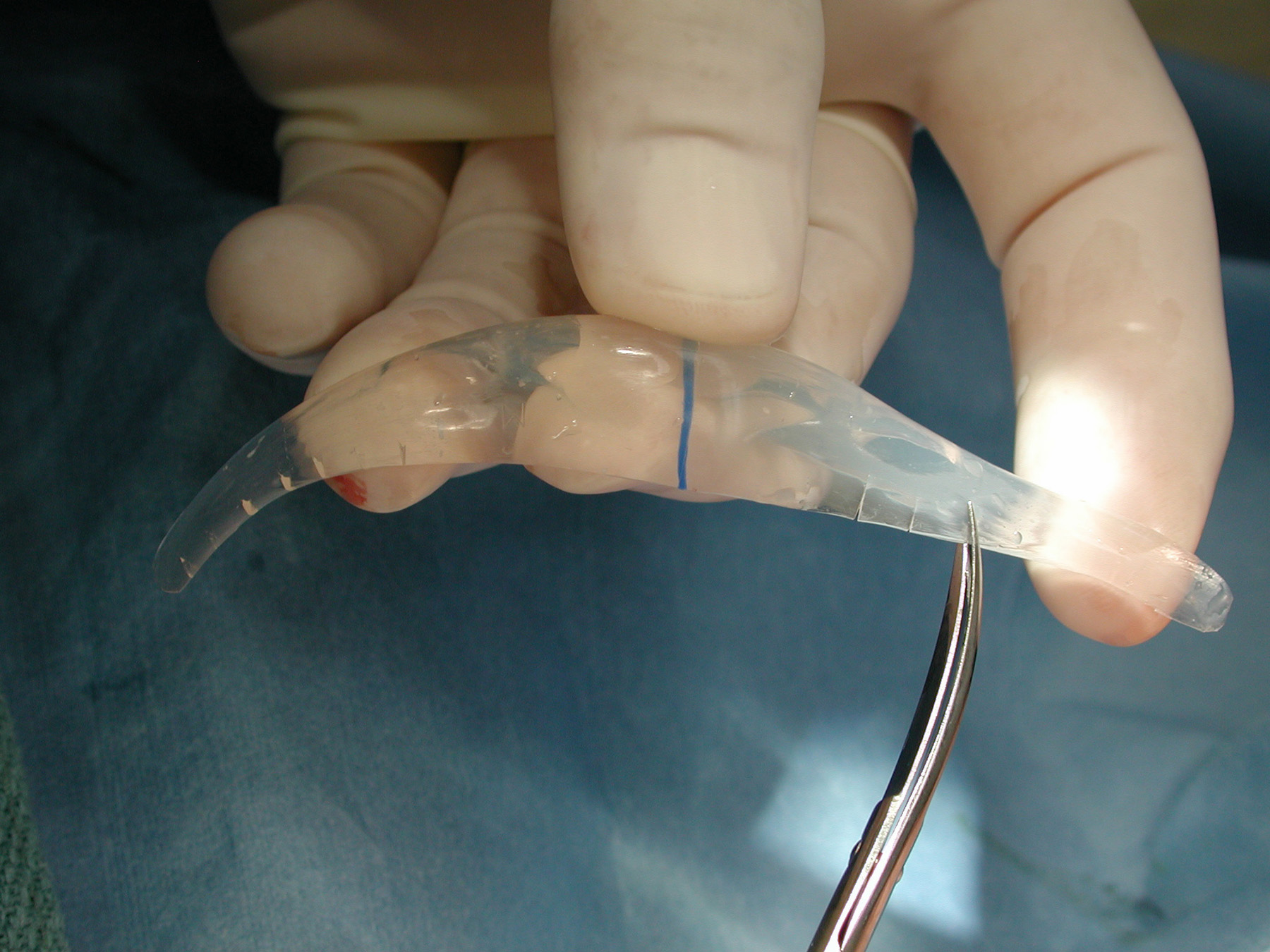 One question that interested me is whether chin implants can become fractured or fragmented from traumatic impact. None of the manufacturers could provide any information about this potential. Therefore, testing was performed using the ASTM (American Society of Testing Materials) drop test. I have previously used this method to test the fracture potential for cranioplasty materials. Using an 8 lb. weight dropped from five feet, silicone, PTFE (Gore-tex) and Medpor chins were tested. Silicone and PTFE implants were unaffected, a Medpor chin did fracture.
One question that interested me is whether chin implants can become fractured or fragmented from traumatic impact. None of the manufacturers could provide any information about this potential. Therefore, testing was performed using the ASTM (American Society of Testing Materials) drop test. I have previously used this method to test the fracture potential for cranioplasty materials. Using an 8 lb. weight dropped from five feet, silicone, PTFE (Gore-tex) and Medpor chins were tested. Silicone and PTFE implants were unaffected, a Medpor chin did fracture.
This test, however, does not really replicate what would happen in human implantation. With the implant up against the bone, the impacting force is transmitted to the underlying bone. As a result, the implant does not absorb the entire force alone or without the support of an underlying framework. Therefore, implant fracture is highly unlikely unless the impacting force is of such a magnitude that the bone would fracture.
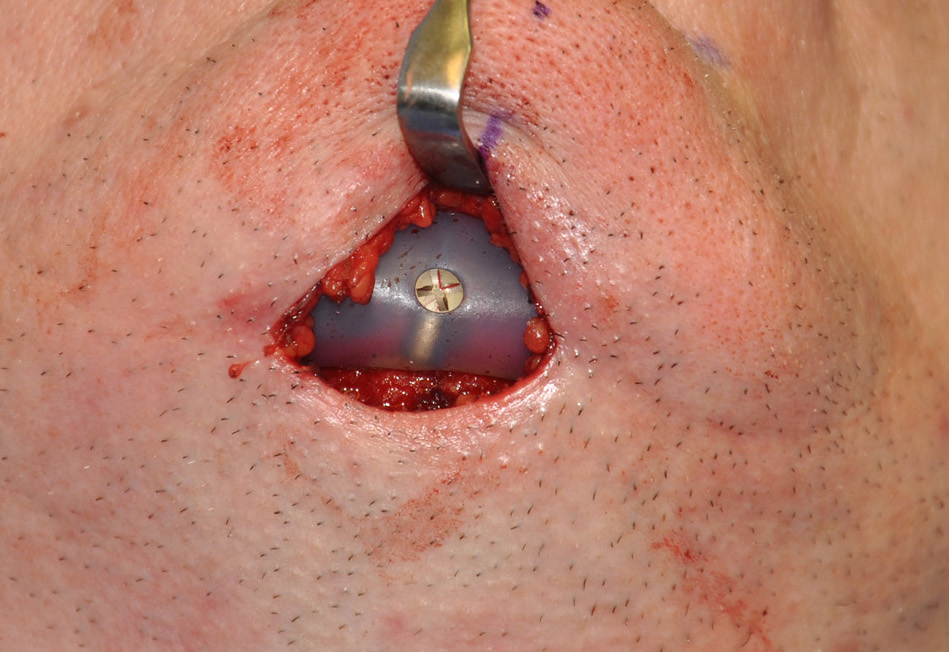 Chin implant shifting or migration, however, is a well known complication. It can occur even in the absence of trauma. It would make sense therefore to protect the implant from that potential in the young athletic male or female. This can be done by single or double screw fixation technique.
Chin implant shifting or migration, however, is a well known complication. It can occur even in the absence of trauma. It would make sense therefore to protect the implant from that potential in the young athletic male or female. This can be done by single or double screw fixation technique.
 By placing two screws through the implant to the underlying bone in a parasagittal fashion, it would be virtually impossible for it to ever shift position after surgery. One could argue that a single midline screw is sufficient, but it is just as easy to place two screws as one.
By placing two screws through the implant to the underlying bone in a parasagittal fashion, it would be virtually impossible for it to ever shift position after surgery. One could argue that a single midline screw is sufficient, but it is just as easy to place two screws as one.
If a patient is concerned about their risk of chin implant problems from athletic participation, screw fixation is a simple prevention measure. They can be easily placed whether the implant is placed through an intraoral or a submental approach.
Dr. Barry Eppley
Indianapolis, Indiana