

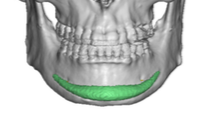
The placement of chin implants can be through either an external submental skin incision or an internal intraoral mucosal incision. Regardless of the incisional approach a subperiosteal tissue pocket has to be created in which the implant will sit. Given the height of most chin implants there is a lot of bone surface area in which the implant can be placed in a north-south or vertical orientation.
 The only commonly recognized limitation of this vertical tissue pocket development is the mental nerve which is most relevant in the lateral pocket dissection. Despite the anatomic knowledge of where the mental nerve is I have seen many a 3D CT scan which shows the wings of a chin implant abutting right up against the nerve or even placed above it. And, by far, chin implants are frequently malpositoned superiorly off of the most projecting point of the chin bone. (above the pogonion) It is much more uncommon to see a chin implant sitting too low.
The only commonly recognized limitation of this vertical tissue pocket development is the mental nerve which is most relevant in the lateral pocket dissection. Despite the anatomic knowledge of where the mental nerve is I have seen many a 3D CT scan which shows the wings of a chin implant abutting right up against the nerve or even placed above it. And, by far, chin implants are frequently malpositoned superiorly off of the most projecting point of the chin bone. (above the pogonion) It is much more uncommon to see a chin implant sitting too low.
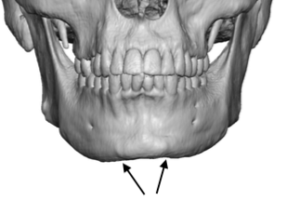
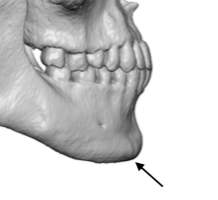 The unrecognized anatomic limitation to good chin implant positioning are the osteocutaneous ligament attachments. They are evident in almost every 3D CT scan of the chin I have seen and appears as raised bumps of bone along the side of the chin. The bone bump appears because of the pull of the ligament on the attached bone surface. It is these ligaments because of their tough attachments that make many surgeons continue their dissection north of them where the tissue elevation is much easier. Continuing along this line of easy line of dissection is why the wings of chin implants can be seen to head north towards the mental nerve rather than back along the inferolateral border of the chin and jawline where they are intended to be placed.
The unrecognized anatomic limitation to good chin implant positioning are the osteocutaneous ligament attachments. They are evident in almost every 3D CT scan of the chin I have seen and appears as raised bumps of bone along the side of the chin. The bone bump appears because of the pull of the ligament on the attached bone surface. It is these ligaments because of their tough attachments that make many surgeons continue their dissection north of them where the tissue elevation is much easier. Continuing along this line of easy line of dissection is why the wings of chin implants can be seen to head north towards the mental nerve rather than back along the inferolateral border of the chin and jawline where they are intended to be placed.
 Release of these osteocutaneous ligaments is the key in chin implant placement. In some patients these releases will be easier than others. (e.g., most women) Once these ligaments are released the dissection becomes very easy along the inferolateral chin and jawline bone. With implants that have long wings this dissection once past the ligamentous attachments can go all the way back to the edge of the masseter muscle.
Release of these osteocutaneous ligaments is the key in chin implant placement. In some patients these releases will be easier than others. (e.g., most women) Once these ligaments are released the dissection becomes very easy along the inferolateral chin and jawline bone. With implants that have long wings this dissection once past the ligamentous attachments can go all the way back to the edge of the masseter muscle.
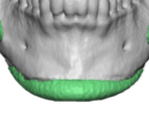
 The osteocutaneous ligaments along the sides of the chin must be released for proper chin implant placement. It not only allows the implant to be positioned where it will have its best effect but also allows the wings of the implant to be asssured of laying flat.
The osteocutaneous ligaments along the sides of the chin must be released for proper chin implant placement. It not only allows the implant to be positioned where it will have its best effect but also allows the wings of the implant to be asssured of laying flat.
Dr. Barry Eppley
Indianapolis, Indiana