

- What influence does the forehead have on one’s appearance?
The forehead is a very prominent and visible facial area. While it is not the most dominant facial feature, it does have an influence on one’s appearance in numerous ways.
The forehead does have an influence on gender appearance. In men, the brow ridge (bossing or prominence above the eyes) is stronger and the forehead angles more steeply away from the eyes. In women, the forehead does not have a prominent brow ridge, tends to be more round, and angles more vertical above the brow rather than more backward sloping as in men.
A forehead can often be seen as too ‘big’ because of the distance between the eyebrows and the frontal hairline. When more than 6.5 cms exists between the two, the forehead will look elongated or large. This may be the result of frontal hairline recession in men or the natural position of the hairline in women.
2. How is forehead reshaping done?
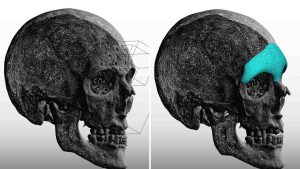
Changing the shape of the forehead can be done in three ways. Brow ridge (bossing) reduction, brow ridge augmentation, or altering the slope or shape of the forehead between the brow bone and the top of the skull under the hairline are the common changes requested.
They all share one common theme, the need to use a coronal or scalp incision for access to do the procedure. This is a more significant aesthetic consideration in men. Surgically changing the brow bone uses different techniques depending upon whether one is reducing or building it up. While some minor bone alterations may be able to be done endoscopically (from above) or through the upper eyelids (from below), major changes require the liberty of unfettered access by the turn down of a scalp flap.
3. How is brow bone reduction done?
In brow bone reduction, the anatomy of the prominent brow must be appreciated. The cause of a prominent brow is that the underlying frontal sinus cavity is expanded. (pneumatized) Because the frontal sinus is air-filled, the prominent brow ridge only has thin bone covering it. It can not just be burred or shaved down in most cases. Only the tail of the brow ridge, where the frontal sinus does not exist, can be simply reduced by shaving.
 In the setback of frontal bossing, the thin plate of overlying must be removed, reshaped, and put back in place with small titanium plates and screws (1mm profile) to hold the bone in place while it heals.
In the setback of frontal bossing, the thin plate of overlying must be removed, reshaped, and put back in place with small titanium plates and screws (1mm profile) to hold the bone in place while it heals.
A plain lateral skull film or cephalometric x-ray will show how much frontal bossing is caused by air vs. actual bone.
4. How is brow bone augmentation done?
Building up a deficient or over-reduced brow ridge requires the use of synthetic materials which are added on top of the bone. The two most commonly used cranioplasty materials are acrylic (PMMA) and hydroxyapatite. (HA) Each material has its own advantages and disadvantages and either one can work in experienced hands.
PMMA incurs less cost to use and has a very high impact resistance. HA is more expensive with a lower impact resistance to trauma. Both can be impregnated with antibiotics and shaped during the procedure. How much material to add and where to place it is very much like sculpting and requires a thorough discussion before surgery with the patient.
 Solid implants, composed of silastic, Gore-tex, or Medpor, can also be used. They require more effort at shaping and must be held in place with tiny titanium screws. Their cost is intermediate between PMMA and HA. Today custom implant design is done to create a brow bone implant that is inserted through an endoscopic approach.
Solid implants, composed of silastic, Gore-tex, or Medpor, can also be used. They require more effort at shaping and must be held in place with tiny titanium screws. Their cost is intermediate between PMMA and HA. Today custom implant design is done to create a brow bone implant that is inserted through an endoscopic approach.
5. Can other areas of the forehead be reshaped besides the brow bone?
The forehead (frontal bone) between the brow ridge and the front of the hairline can also be reshaped. It can be made flatter, more round, narrower, or wider. Changes can be done in either profile, width, or both. This is done through either burring of the prominent areas, adding material on deficient areas, or a combination of both.
6. What is the recovery after forehead reshaping? What complications can occur?
Aesthetic forehead surgery is usually done as an outpatient procedure. Depending upon what other procedures may be done with it, it may require an overnight stay in the surgical facility. A wrap-around forehead dressing is put on at the end of surgery and is removed the next day. In some cases, a drain may be removed (not commonly) and it is removed the next day also. Ther6e is some mild pain afterward but much of the forehead skin will be numb for awhile. Pain is easily controlled by pills. There will be some swelling afterwards which is driven downward by the dressing and gravity which affects the eyes and upper cheeks. It is most evident by two days after surgery and is largely gone within seven to ten days after surgery. Most patients return to work in two to three weeks. Dissolveable sutures are used in the scalp so there is no need for suture remocal. One can return to working out in two weeks after surgery.
Complications of significance are very rare with forehead surgery. The forehead skin will be numb but normal feeling will return in most patients within six to eighty weeks after surgery. It is possible to not get back all of your feeling. The biggest concern is aesthetic…did we achieve what our goal was? Is the forehead contour smooth and even? Is it too much or too little?
7. What can I do if my forehead is too long?
Usually a long forehead is a female concern. It is evident when the distance between the eyebrows and the frontal hairline is aesthetically too long, usually greater than 6.5 or 7cms in length.
The length or size of the forehead skin can be reduced by a scalp advancement (hairline lowering. This is conceptually a ‘reverse browlift’. An incision is made at the frontal hairline and the scalp behind it is loosened and brought forward over the fixed forehead skin. The underlying forehead skin is then removed and the hairline closed in its new lower position. A frontal hairline can be advanced between 1 and 2.5 cms, which often makes for a significant difference.
Dr. Barry Eppley
Indianapolis, Indiana