

 Buttock augmentation has evolved over the last two decades in two different volumetric treatment approaches. Injectable fat grafting has become the most common method of buttock augmentation due to the combined benefits of reductive body contouring and gluteal enlargement. Concurrently, buttock implant techniques have evolved with intramuscular pocket locations and improved implant materials and sizes and shapes. Because of the more invasive nature of implant placement, this alloplastic method remains limited to those who have inadequate fat for injection grafting. Each method of buttock augmentation, however, has their own distinct advantages and disadvantages.
Buttock augmentation has evolved over the last two decades in two different volumetric treatment approaches. Injectable fat grafting has become the most common method of buttock augmentation due to the combined benefits of reductive body contouring and gluteal enlargement. Concurrently, buttock implant techniques have evolved with intramuscular pocket locations and improved implant materials and sizes and shapes. Because of the more invasive nature of implant placement, this alloplastic method remains limited to those who have inadequate fat for injection grafting. Each method of buttock augmentation, however, has their own distinct advantages and disadvantages.
The disadvantages of buttock fat grafting can include aesthetic issues of loss of grafted volume, contour irregularities/asymmetries, and fat necrosis/oil cysts. But it has also become apparent that serious medical complications can also occur in rare cases which is pulmonary fat embolism resulting in lung dysfunction and even death has occurred. Avoiding injecting fat into the gluteal muscle has been shown to significantly lower and even largely eliminate this medical risk.
The disadvantages to buttock implant placement is like implant placement anywhere on the body which sharply contrasts with that of fat injections. While the volume implanted is permanent it is a more invasive procedure which has a risk of infection and aesthetic implant-related issues. Compared to any other form of body implants, however, buttock implants are a harder recovery given their location and the role that the buttocks play in both sitting and walking.
In the December 2019 issue of the journal Plastic and Reconstructive Surgery an article was published on this topic entitled ‘Composite Buttock Augmentation: The Next Frontier in Gluteal Aesthetic Surgery.’ In this clinical paper the authors report on their experience with one hundred and forty-seven (147) cases of composite buttock augmentation with an average of eighteen (18) months followup. Composite buttock augmentation is defined as combining buttock implants with fat grafting. Specifically the buttock implants are placed in an intramuscular pocket with overlying injection of fat in the subcutaneous space.
Operative times averaged just under two hours. Average implant volume was 300ccs (180ccs to 370ccs) with average injected fat volume per side of 380ccs. (80ccs to 900ccs) Fat injections were done prior to implant placement but after intramuscular pocket dissection. Overall complication rates were close to 12%. The most common complication was implant dislocation (due to the use of anatomical implants, none occurred with round implants) and loss of adequate muscle coverage due to muscle thinning (7%) Infection occurred in seven patients. (5%) None of the infections were related to the fat grafting.

 The authors described several important implant-related observations that are well known to plastic surgeons that have done a lot of buttock implants in both the subfascial and intramuscular locations. First, the dissection of the intramuscular pocket is not done in a natural tissue plane like that of submuscular breast implants. It is an artificially created pocket done the midst of the gluteus major muscle. Learning how to get deep enough into the muscle to keep a viable thickness of the muscle layer over the implant is a learned skill. It is not intuitive and the natural tendency is to make the intramuscular dissection not deep enough for fear of the location of the sciatic nerve, resulting in a thin muscle layer over the implant that eventually atrophies. This then has the implant end up with inadequate soft tissue coverage over time. (resulting in implant displacement/show)
The authors described several important implant-related observations that are well known to plastic surgeons that have done a lot of buttock implants in both the subfascial and intramuscular locations. First, the dissection of the intramuscular pocket is not done in a natural tissue plane like that of submuscular breast implants. It is an artificially created pocket done the midst of the gluteus major muscle. Learning how to get deep enough into the muscle to keep a viable thickness of the muscle layer over the implant is a learned skill. It is not intuitive and the natural tendency is to make the intramuscular dissection not deep enough for fear of the location of the sciatic nerve, resulting in a thin muscle layer over the implant that eventually atrophies. This then has the implant end up with inadequate soft tissue coverage over time. (resulting in implant displacement/show)
 Their second implant-related observation is that, while the use of anatomically shaped implants has their aesthetic ppeal, they have a far greater risk of displacement and asymmetry which is largely avoided with the use of round implants.
Their second implant-related observation is that, while the use of anatomically shaped implants has their aesthetic ppeal, they have a far greater risk of displacement and asymmetry which is largely avoided with the use of round implants.
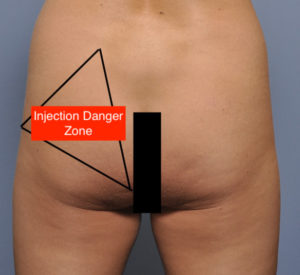
 Where the injection fat grafting techniques differs, besides avoiding intramuscular fat placement, is the lateralization of the injections. This keeps the injected fat out of the danger zone even if placed in the subcutaneous plane. Equally importantly it focuses the available fat to where the implant does not create a volume effect closer to the hips, the known limitation of intramuscular implant placement.
Where the injection fat grafting techniques differs, besides avoiding intramuscular fat placement, is the lateralization of the injections. This keeps the injected fat out of the danger zone even if placed in the subcutaneous plane. Equally importantly it focuses the available fat to where the implant does not create a volume effect closer to the hips, the known limitation of intramuscular implant placement.
The periprosthetic buttock augmentation concept is that the implant provides a permanent core of intramuscular volume while the fat adds more volume as well as thickens the overlying subcutaneous fat layer. In essence this combines the best of both buttock augmentation methods while decreasing the reliance on either one alone…which is where the risk of complications increases. (bigger implants in the subfascial location and very large volumes of injected fat)
Dr. Barry Eppley
Indianapolis, Indiana