

Temporal artery ligation refers to tying off the superficial temporal artery, the vessel in the temple/scalp region. It is not the treatment for temporal arteritis / giant cell arteritis (GCA) which historically was treated by temporal artery excisional biopsy.
Cosmetic temporal artery ligation is a minor surgical procedure used to eliminate visible, pulsatile superficial temporal artery branches in the temple that patients find aesthetically undesirable. These arteries can become prominent with aging, low body fat, exercise, heat exposure, or prior facial surgery.
Anatomy
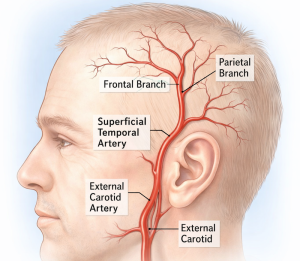 The superficial temporal artery (STA) is a terminal branch of the external carotid artery. After crossing the zygomatic arch, it divides into:
The superficial temporal artery (STA) is a terminal branch of the external carotid artery. After crossing the zygomatic arch, it divides into:
- Frontal branch
- Parietal branch
The frontal branch is responsible for the visible pulsating vessel across the temple or forehead.
Common Symptoms
Patients usually complain of:
- Visible pulsating vessel in the temple
- A rope-like artery across the side of the forehead
- Prominence during exercise, heat or alcohol intake
- Rarely associated with temporal headaches
- Concerns after facelift or fat loss
It is especially common in thin, athletic, or older patients.
Surgical Concept
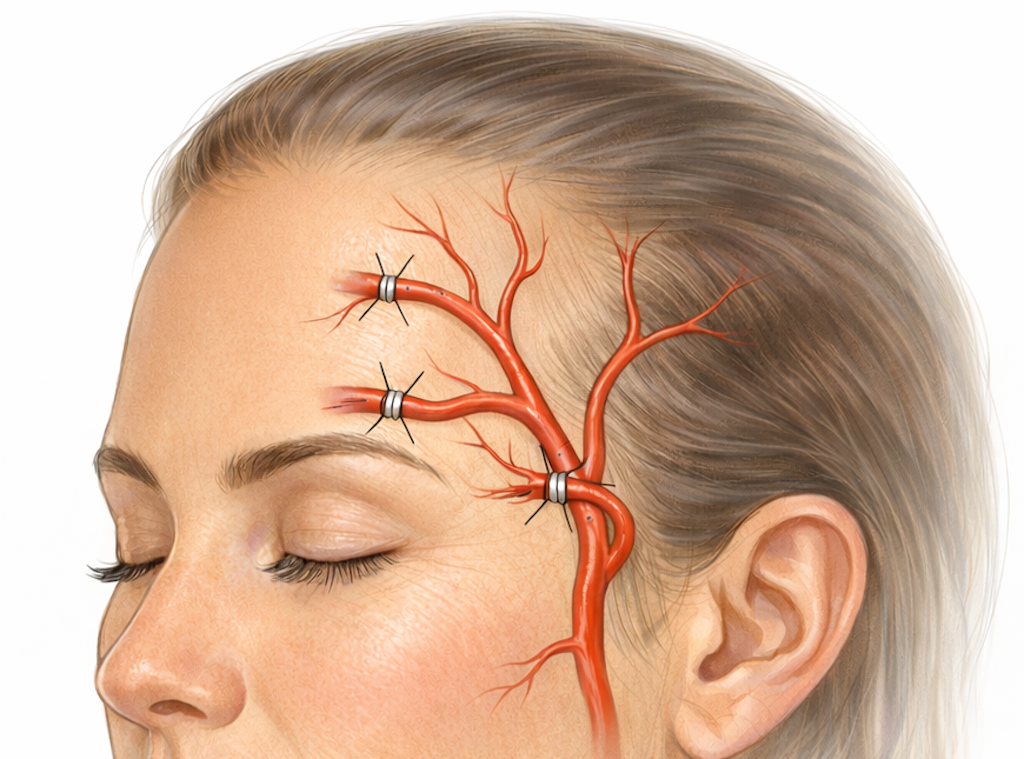
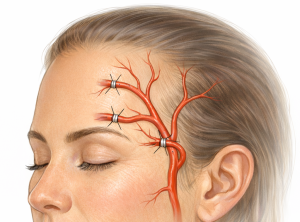
Under local anesthesia through multiple ascending small incision the arterial branch is carefully dissected and doubly ligated or clipped. The exposed arterial segment can be tied and cut but I not found that to be necessary
The small incisions aer closed with very small dissolvable sutures.
Total treatment time is 60 to 90 minutes.
Results are immediate once swelling resolves.
Why Ligation Works
The scalp has extensive collateral circulation from:
- Contralateral superficial temporal artery
- Occipital artery
- Posterior auricular artery
- Supraorbital/supratrochlear arteries
Therefore eliminating a branch does not compromise scalp perfusion or hair viabilty/growth.
Advantages
- Permanent removal of visible vessel
- Very small scars (some are hidden in hairline)
- Local anesthesia
- Quick recovery
Risks / Complications
Although very uncommon:
- Bruising or hematoma (not yet seen)
- Temporary scalp numbness (not yet seen)
- Scar visibility (no one has complained about that to date)
- Recurrence if vessel not fully excised (1% to 2% risk)
- Injury to temporal branch of facial nerve if dissection goes too deep (not yet seen)
Alternative Treatments
Some surgeons attempt:
- Laser therapy
- Sclerotherapy
However, arteries are high-flow vessels, so these methods are less reliable and may risk embolization or skin injury.
For that reason, ligation/excision is considered the most definitive treatment.
Case Study

 This older male developed prominent superficial temporal arteries as he had gotten older. He was thin with mild temporal and submalar hollowing. On his right side there was the typical visible serpiginous course of the artery. On his left side the artery was bigger and largely straight. (temporal artery asymmetry)
This older male developed prominent superficial temporal arteries as he had gotten older. He was thin with mild temporal and submalar hollowing. On his right side there was the typical visible serpiginous course of the artery. On his left side the artery was bigger and largely straight. (temporal artery asymmetry)

 Under local anesthesia three small incisions were made along the course of the artery. The most proximal incision was where the artery left the temporal hairline. The most distal incision was placed at the side of the forehead where the artery always takes a 90 degree turn up into the frontal hairline. And a third incision was placed between the two.
Under local anesthesia three small incisions were made along the course of the artery. The most proximal incision was where the artery left the temporal hairline. The most distal incision was placed at the side of the forehead where the artery always takes a 90 degree turn up into the frontal hairline. And a third incision was placed between the two.
 Through these incisions the artery was dissected out at these three incisions and double ligated.
Through these incisions the artery was dissected out at these three incisions and double ligated.
 Interestingly on the left side with the straighter artery it was nearly twice as big as the artery on the right side.
Interestingly on the left side with the straighter artery it was nearly twice as big as the artery on the right side.

 With just three ligations per side the arterial flow was eliminated as confirmed by the lack of a doppler signal.
With just three ligations per side the arterial flow was eliminated as confirmed by the lack of a doppler signal.
Discussion
In cosmetic temporal artery ligation (for prominent superficial temporal arteries), the number of ligation points typically depends on the arterial pattern and branches, but there are common ranges used in practice.
Typical Number of Ligation Points
- Minimum: 3 ligations
- Most common: 3–4 ligations
- Occasionally: 5 ligations if additional feeder branches exist.
Why Multiple Ligations Are Needed
 A single ligation usually fails because blood can still enter the vessel through retrograde flow from distal branches or collateral vessels. Therefore both inflow and backflow must be stopped.
A single ligation usually fails because blood can still enter the vessel through retrograde flow from distal branches or collateral vessels. Therefore both inflow and backflow must be stopped.
Common Cosmetic Technique (for anterior branch of STA)
Typical multilevel approach:
- Proximal ligation
- Near or at the temporal hairline of the superficial temporal artery.
- Middle ligation
-
- Usually at the “elbow” or bend of the artery in the lateral forehead.
- Distal ligation
-
- Near the upper visible end of the artery in the forehead.
This three-point ligation is commonly required for optimal cosmetic elimination of the vessel. But one must always be prepared to do more.
Situations Requiring More
- Accessory or duplicated branches
- Early branching before the Y split
- Persistent Doppler signal after 3 ligations
In these cases, a fourth ligation lower on the arterial trunk may be added to eliminate remaining inflow.
Dr Barry Eppley
Plastic Surgeon