

Introduction
Custom Infraorbital–malar implants are facial implants designed to augment the under-eye (infraorbital) region and the cheekbone (malar) area simultaneously. Such implant designs are only available by custom fabrication in which they fitted to match the patient’s unique skeletal anatomy based on 3-D CT scan imaging.They are most commonly used to correct:
- Flat or weak midface projection
- Under-eye hollowing
- Negative orbital vectors
- Midface deficiency from genetics, aging, trauma, or prior surgery
- Residual deformities after Le Fort or orbital reconstruction
A custom infraorbital–malar implant typically spans:
- Infraorbital rim (the lower eye socket border)
- Zygomatic–malar body (the front part of the cheekbone)
- Optional extensions to:
- Zygomatic arch (lateral cheekbone)
- Pyriform aperture (upper maxilla)
- Orbital floor edges (for rim-floor blending)
This creates a continuous, smooth augmentation across the lower eyelid and cheek—something off-the-shelf implants simply can not do.
The benefits of custom infraorbital-malar implants include:
1. Full Anatomic Fit
- Designed from the patient’s CT scan
- Mirrors the native contour for a seamless fit
- Reduces asymmetry
2. Fills the “under-eye–cheek transition”
This area is notoriously hard to correct with fillers or fat alone. Custom implants allow:
- Correction of tear-trough hollowing
- Support of the lower eyelid
- Better anterior cheek projection
3. Ability to Correct Asymmetry or Abnormalities
Such as:
- Orbital asymmetry/dystopia
- Enophthalmos-like appearance from midface deficiency
- Post-traumatic contour irregularities
4. Predictable, Long-Term Correction
Unlike fillers, implants offer:
- Permanent augmentation
- No resorption like fat
- Highly stable results
Patients often seek custom infraorbital–malar implants for:
- Sunken eyes / prominent lower eyelid bags caused by lack of skeletal support
- Weak cheekbones
- Deep tear troughs
- “Flat” or under-projected midface
- Fixing asymmetry
- Negative orbital vector anatomy (cheek behind lower lid)
Case Study

 This middle-aged male had fat injection grafting to the lower eyelids and cheeks for augymentatiojk which was unsuccessful. It left him with multiple fat lumps and irregularities of the eyelids and no significant rim or cheek augmentation.
This middle-aged male had fat injection grafting to the lower eyelids and cheeks for augymentatiojk which was unsuccessful. It left him with multiple fat lumps and irregularities of the eyelids and no significant rim or cheek augmentation.
![]()
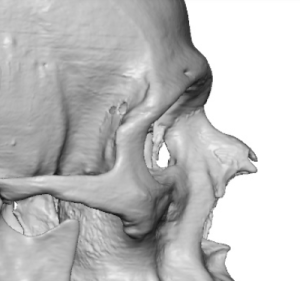
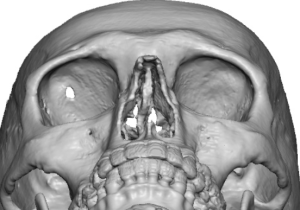 His 3D CT scan showed moderate infraorbital and cheek horizontal deficiency on top of a mild to moderate midface hypoplasia.
His 3D CT scan showed moderate infraorbital and cheek horizontal deficiency on top of a mild to moderate midface hypoplasia.
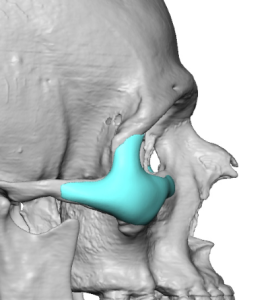
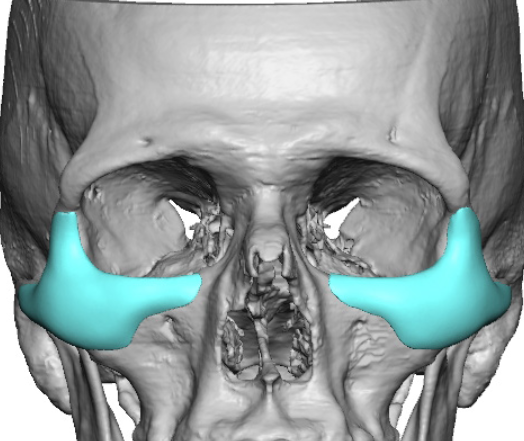
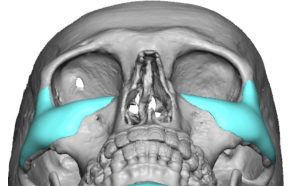 Custom infraorbital-malar implants were designed which saddled the orbital rim and raised it 4mms. Malar projection was 3.5mms. Implant volumes were 3.1ccs per side.
Custom infraorbital-malar implants were designed which saddled the orbital rim and raised it 4mms. Malar projection was 3.5mms. Implant volumes were 3.1ccs per side.
 Through subciliary lower eyelid incisions the numerous fat lumps were exposed and removed.
Through subciliary lower eyelid incisions the numerous fat lumps were exposed and removed.
 The custom implants when placed on the patient seemed improbable to fit through the incisions. But with persistence and care it is always possible.
The custom implants when placed on the patient seemed improbable to fit through the incisions. But with persistence and care it is always possible.

 The implants were secured with microscrews at the upper zygomatic eminence. With eyelid closure lateral canthopexies were performed.
The implants were secured with microscrews at the upper zygomatic eminence. With eyelid closure lateral canthopexies were performed.
Discussion
These two different approaches to the treatment of orbital and malar deficiencies (custom infraorbital–malar implants vs fat injection grafting can be compared as follows.
1. Goals: Volume vs Structural Projection
Custom Implants
- Provide skeletal projection, not soft-tissue volume.
- Extend the bone framework forward/outward.
- Correct:
- Midface deficiency
- Negative vector
- Infraorbital support insufficiency
- Asymmetry
- Under-eye hollowing from bone deficiency
Fat Grafting
- Provides soft-tissue fullness, not skeletal projection.
- Fills hollows and softens transitions.
- Best for mild–moderate volume deficiency, especially soft-tissue related.
Key difference:
Implants augmenty bone structure ? shape change
Fat augments soft tissue ? fullness change
2. Degree of Enhancement
Custom Implants
- Can make large, precise, and sharp midface changes.
- Enhances:
- Cheek contour
- Orbital rim support
- Lid–cheek blending
- Customization allows asymmetric correction down to fractions of a millimeter.
Fat Grafting
- Better for subtle or moderate fullness.
- Cannot create angular, sculpted cheek shapes.
- Overfilling the under-eye leads to puffiness or irregularities.
3. Longevity
Custom Implants
- Permanent.
- Stable shape and volume for life unless removed/changed.
Fat Grafting
- Unpredictable: 30–70% long-term retention on average.
- May require repeat sessions.
- Fat can change with body weight, aging, or metabolic factors.
4. Predictability
Custom Implants
- Highly predictable due to 3-D CT design.
- Results are almost identical to the digital plan.
Fat Grafting
- Least predictable of all midface augmentation methods.
- Variables include:
- fat survival
- vascularity
- patient metabolism
- surgeon technique
5. Lower Eyelid Support
Custom Implants
- The best method to structurally support the lower eyelid and tear-trough area.
- Particularly beneficial in:
- negative vector anatomy
- scleral show
- weak infraorbital rims
- Reduces hooding or hollowing due to lack of bony support.
Fat Grafting
- Provides almost no structural support.
- May even worsen lower eyelid contour if placed too superficially.
6. Recovery
Custom Implants
- 7–14 days for visible swelling; full settling 6–12 weeks.
- Longer downtime than fat but usually one-and-done.
Fat Grafting
- Minimal downtime (2–4 days).
- Swelling and asymmetry common for 2–3 weeks.
- May need touch-ups later.
7. Risks
Custom Implants
- Implant malposition (rare with screw fixation)
- Edge visibility if design is poor (solved with custom blending)
- Infection (low but possible)
- Need for precise surgical technique
Fat Grafting
- Asymmetry or under-correction
- Visible lumps/irregular texture, especially near the lower eyelid
- Overgrowth (rare, but fat can hypertrophy with weight gain)
- Unpredictable long-term outcome
- Rare intravascular injection risk (not seen with midface implants)
8. Ideal Candidates
Custom Infraorbital–Malar Implants
Best for patients with:
- Structural midface deficiency
- Sunken infraorbital rims
- Strong negative vector
- Chronic under-eye hollowing resistant to fillers/fat
- Desire for sharper cheek projection
- Asymmetry or prior trauma
Fat Grafting
Best for patients with:
- Mild hollowing
- Good eyelid–cheek support
- Wanting a softer, natural fullness
- Not needing a strong contour or skeletal augmentation
Summary Chart
|
Feature |
Custom Implants |
Fat Grafting |
|
Type |
Structural / bone augmentation |
Soft-tissue volume |
|
Longevity |
Permanent |
Variable |
|
Predictability |
Very high |
Low–moderate |
|
Lower eyelid support |
Excellent |
Minimal |
|
Sculpted cheeks |
Excellent |
Poor |
|
Downtime |
Moderate |
Low |
|
Revisions needed |
Rare |
Often |
|
Best for |
Structural deficiency |
Minor hollowing |
Key Points
- Fat grafting is prone to contour irregularities when used over and around the orbital rim area where thin overlying tissues exist.
- The only effective treatment for infraorbital-malar recession is a ‘wrap around’ upper midface implant design of which the Type 1 infraorbital-malar implant design is most commonly used.
- Placed through a limited lower eyelid incision microscrew fixation and lateral canthopexies are used for implant stability and lower eyelid support.
Dr. Barry Eppley
World-Renowned Plastic Surgeon