

Facial asymmetry is common and it is often said that everyone has some degree of it. While this is true, more significant facial asymmetries are not common and are a source of frequent patient self-esteem issues. In significant facial asymmetries the entire face is affected from the brow down to the jawline. The affected side is almost always lower as if it is pulled downward. It is extremely rare to ever see a facial asymmetry where the affected side is higher rather than lower than the normal side
The most significant component of facial asymmetry is often around the eye area. This is usually manifest by a difference in the horizontal level of the pupils. The eyeball sits lower as the orbital floor is located more inferior than the opposite normal side. But the orbital floor is not the culprit but a symptom of the overall facial asymmetry. The entire orbitozygomatic bony complex is situated lower. This is seen by the presence of a smaller and less projected cheek and greater soft tissue fullness below the cheek.
In correcting the orbital or midfacial component of facial asymmetry, orbital floor and cheek augmentation are the two skeletal components of the problem that needs to be addressed. There are a variety of materials and methods to this type of skeletal augmentation and all can be successful when done well.
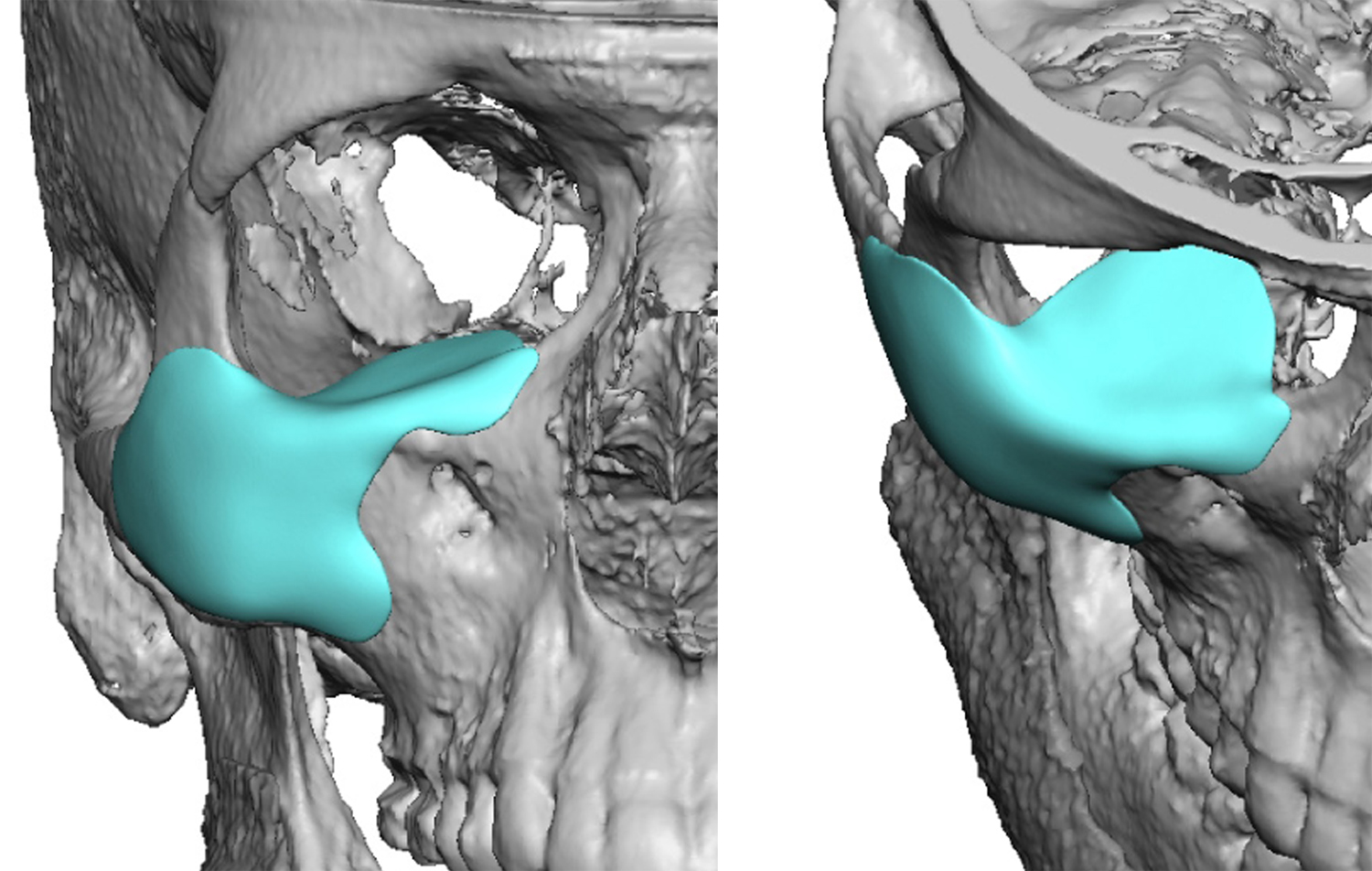
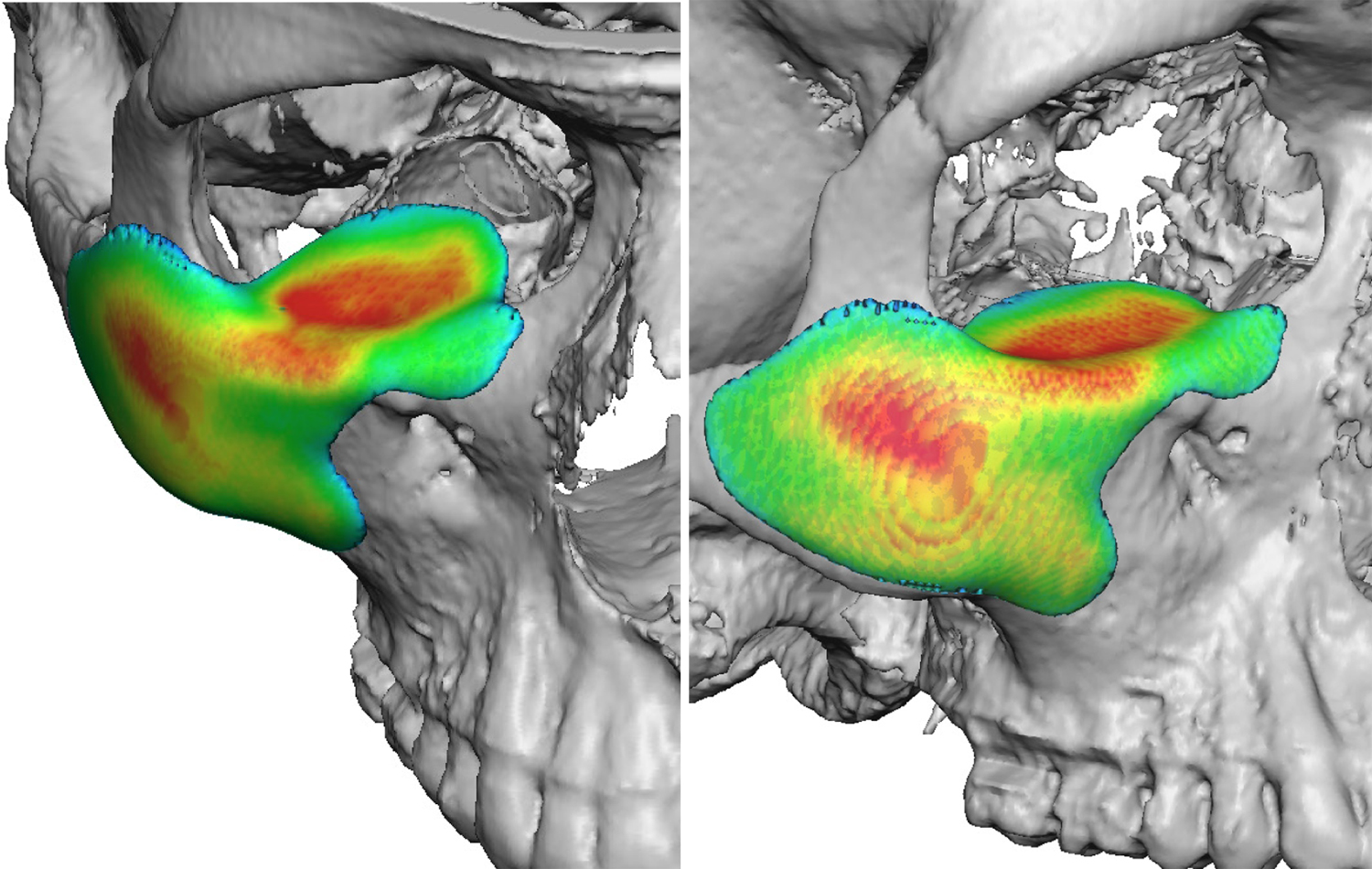 The more recent availability and use of 3D CT scan imaging and computer designing, however, brings greater precision to the level of the surgical result obtainable for orbito-zygomatic reconstruction in facial asymmetry. Comparing the lower side to the higher normal side allows for an implant that can create a bony augmentation that matches to the other side with millimeter precision. In addition a total one-piece implant can be made that augments all outer areas of the bone including the infraorbital and lateral orbital rim. This would be the most accurate method of implant reconstruction available.
The more recent availability and use of 3D CT scan imaging and computer designing, however, brings greater precision to the level of the surgical result obtainable for orbito-zygomatic reconstruction in facial asymmetry. Comparing the lower side to the higher normal side allows for an implant that can create a bony augmentation that matches to the other side with millimeter precision. In addition a total one-piece implant can be made that augments all outer areas of the bone including the infraorbital and lateral orbital rim. This would be the most accurate method of implant reconstruction available.
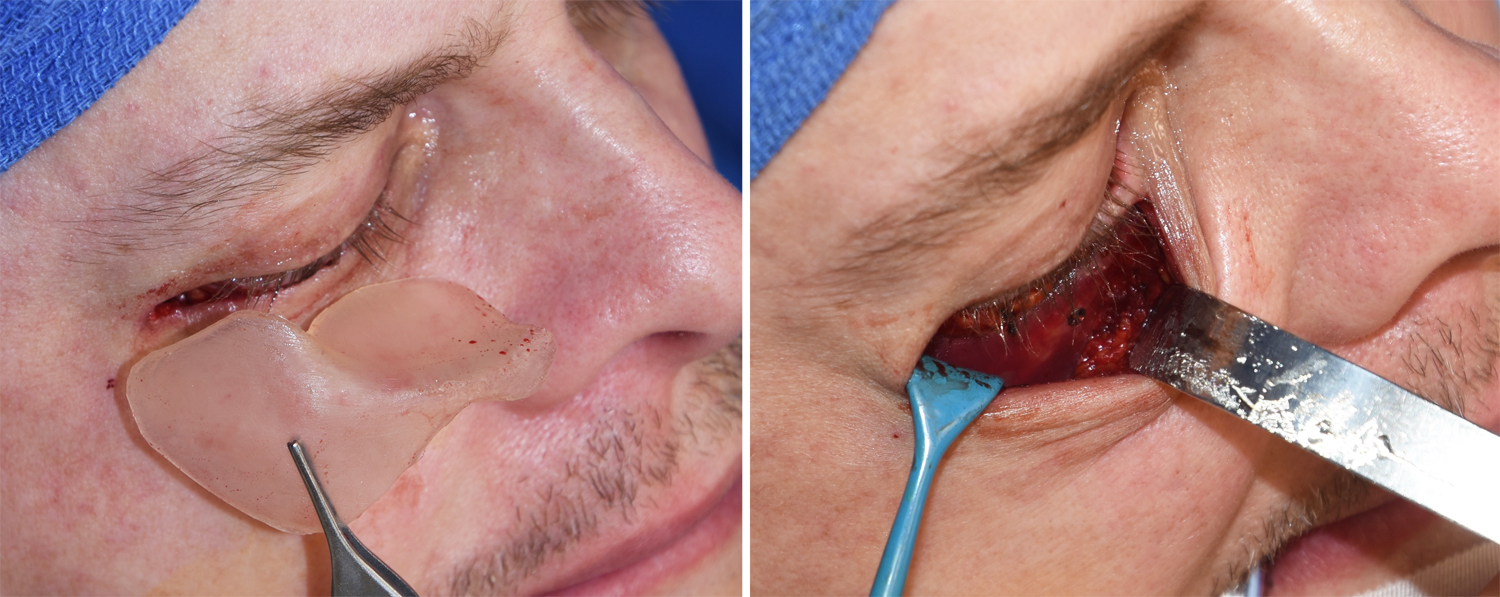
 A custom orbitozygomatic implant is placed through a lower blepharoplasty incision. This is a subciliary incision with a small lateral canthal extension. A skin-muscle flap is raised down to the bone where subperiosteal undermining is done to placed the implant. It is important on closure that the orbicularis muscle suspension is done as well as closing the deeper tissue layer over the lateral orbital rim.
A custom orbitozygomatic implant is placed through a lower blepharoplasty incision. This is a subciliary incision with a small lateral canthal extension. A skin-muscle flap is raised down to the bone where subperiosteal undermining is done to placed the implant. It is important on closure that the orbicularis muscle suspension is done as well as closing the deeper tissue layer over the lateral orbital rim.
It is important to recognize that a custom orbitozygomatic implant provides bone correction but the overlying soft tissues of the eye must often be addressed as well. These could include lateral canthoplasty for outer corner of the eye correction as well as potential upper eyelid ptosis repair. As the eyeball is lifted a ptosis may be created as the upper eyelid position will not have changed. This eyelid correction should be corrected secondarily three months later when all the swelling has resolved and the tissues have stabilized.
Dr. Barry Eppley
Indianapolis, Indiana