

Eye asymmetry can result from differences in the shape of the bony socket in which the eyeball resides. The eye sits within a cone-shaped cylinder of bone that is widest in the front—where the cornea, iris, and sclera are visible—and narrows at the back to a small opening for the optic nerve to pass into the brain. Variations in the position or size of this bony structure between the two sides account for many cases of eye asymmetry.
The orbital bones, much like the optic vesicles, begin developing by the third month in utero. They converge toward the midline as the face forms, continuing this process up until birth. Given the complexity of their growth, it is remarkable that most people develop relatively symmetrical eye positions. However, asymmetries do occur, with one of the most common being a vertical difference in orbital bone position. When one orbit sits lower than the other, the condition is known as vertical orbital dystopia (VOD). Most often, VOD presents on the right side, with horizontal pupillary differences of 5 mm or less being the most typical.
Surgical Correction
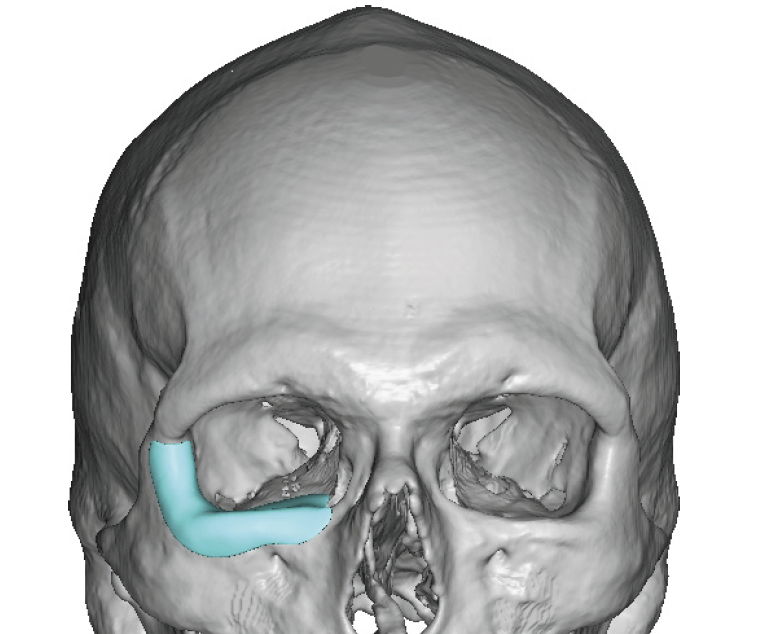
 Correcting VOD requires addressing both the orbital bones and the surrounding soft tissues. While repositioning the lower orbital floor and rim is part of the procedure, augmenting the bone to elevate the lower eyeball is the cornerstone of treatment. This can be precisely planned using a 3D CT scan of the face.
Correcting VOD requires addressing both the orbital bones and the surrounding soft tissues. While repositioning the lower orbital floor and rim is part of the procedure, augmenting the bone to elevate the lower eyeball is the cornerstone of treatment. This can be precisely planned using a 3D CT scan of the face.
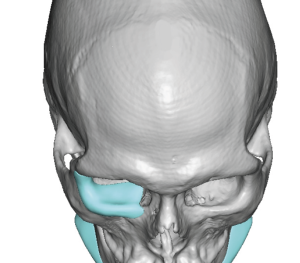
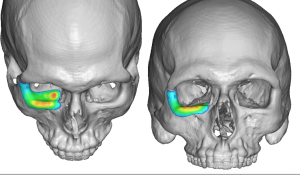 In nearly all cases, it is not just the orbital floor and infraorbital rim that are lower, but the entire orbital “box.” This difference can be both seen clinically and measured with precision, which allows for the design of a custom orbital implant. The implant is created by mirroring the higher, unaffected side onto the lower side of the 3D scan. From this, the implant’s surface coverage and thickness are determined. For example, in one design, areas shown in red represent 4 mm thickness while blue areas represent 1 mm. Such accuracy is possible only through custom fabrication.
In nearly all cases, it is not just the orbital floor and infraorbital rim that are lower, but the entire orbital “box.” This difference can be both seen clinically and measured with precision, which allows for the design of a custom orbital implant. The implant is created by mirroring the higher, unaffected side onto the lower side of the 3D scan. From this, the implant’s surface coverage and thickness are determined. For example, in one design, areas shown in red represent 4 mm thickness while blue areas represent 1 mm. Such accuracy is possible only through custom fabrication.
Implant Placement

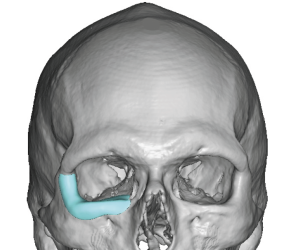
 The implant is inserted through a subciliary lower eyelid incision. After lifting the orbital contents off the bony rim, the implant is slid into place and aligned with the orbital rim according to the preoperative design. Surgeons are often surprised by the actual size of the implant compared to its digital design. Once positioned, the implant is secured to the orbital rim using microscrews.
The implant is inserted through a subciliary lower eyelid incision. After lifting the orbital contents off the bony rim, the implant is slid into place and aligned with the orbital rim according to the preoperative design. Surgeons are often surprised by the actual size of the implant compared to its digital design. Once positioned, the implant is secured to the orbital rim using microscrews.
![]()
 It is critical to confirm that the orbital contents are not entrapped, particularly at the implant’s posterior edge. Once the contents rest freely over the implant, a spacer graft can be placed between the tarsus and the open edge of the split orbicularis muscle. This vertically lengthens the lower eyelid, preventing scleral show as the eyeball is elevated. Because of this, lower lid adjustment is required in almost every VOD correction. Otehr adjuctive procedures may be needed as well including lateral canthoplasty and upper eyelid elevation for a total VOD correction.
It is critical to confirm that the orbital contents are not entrapped, particularly at the implant’s posterior edge. Once the contents rest freely over the implant, a spacer graft can be placed between the tarsus and the open edge of the split orbicularis muscle. This vertically lengthens the lower eyelid, preventing scleral show as the eyeball is elevated. Because of this, lower lid adjustment is required in almost every VOD correction. Otehr adjuctive procedures may be needed as well including lateral canthoplasty and upper eyelid elevation for a total VOD correction.
Comprehensive Treatment
 I wish the correction of VOD was as ‘simple’ as the placement of a custom orbital implant but in the majority of cases it is not Management of VOD typically requires multiple coordinated procedures. The primary operation is placement of a custom orbital implant, precisely designed from the patient’s 3D CT scan to elevate the eye. Secondary procedures, such as eyelid adjustments, are performed in harmony with the bony correction to achieve improved symmetry and natural appearance.
I wish the correction of VOD was as ‘simple’ as the placement of a custom orbital implant but in the majority of cases it is not Management of VOD typically requires multiple coordinated procedures. The primary operation is placement of a custom orbital implant, precisely designed from the patient’s 3D CT scan to elevate the eye. Secondary procedures, such as eyelid adjustments, are performed in harmony with the bony correction to achieve improved symmetry and natural appearance.
Dr. Barry Eppley
World-Renowned Plastic Surgeon