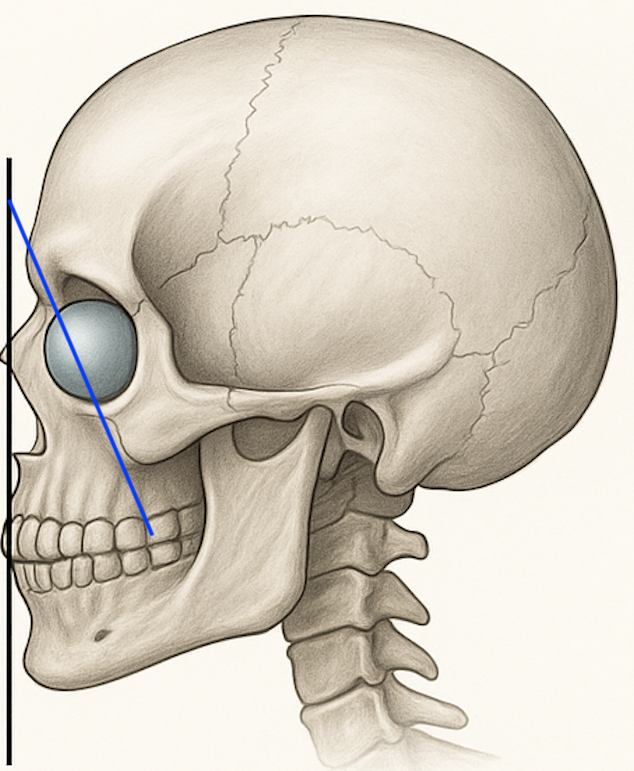


 A negative orbital vector is a not uncommon aesthetic facial deficiency that is often not recognized leading to ineffective treatments. Negative vector midface deformity refers to posterior positioning of the infraorbital rim and anterior maxilla relative to the globe. Clinically, the corneal apex projects anterior to the infraorbital rim in profile view. This skeletal deficiency may contribute to:
A negative orbital vector is a not uncommon aesthetic facial deficiency that is often not recognized leading to ineffective treatments. Negative vector midface deformity refers to posterior positioning of the infraorbital rim and anterior maxilla relative to the globe. Clinically, the corneal apex projects anterior to the infraorbital rim in profile view. This skeletal deficiency may contribute to:
- Tear trough deformity
- Lower eyelid hollowing
- Scleral show
- Poor lower eyelid support
- Midface flatness
Management requires distinguishing between skeletal deficiency, soft tissue descent, and true eyelid laxity. Failure to differentiate these components leads to inappropriate procedures and suboptimal outcomes.
The following presents a structured decision-tree algorithm for evaluation and treatment.
Step 1: Confirm True Negative Vector
Clinical Assessment
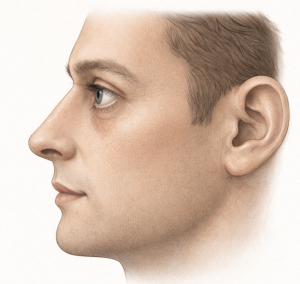
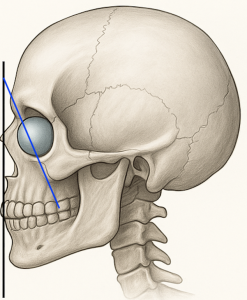
Evaluate in profile:
- Does the globe project anterior to the infraorbital rim?
- Is there infraorbital hollowing?
- Is there scleral show?
Radiographic Confirmation (3D CT)
 Infraorbital rim retrusion (mm relative to globe)
Infraorbital rim retrusion (mm relative to globe)- Anterior maxillary concavity
- Zygomatic projection deficiency
- Asymmetry patterns
 Infraorbital rim retrusion (mm relative to globe)
Infraorbital rim retrusion (mm relative to globe)If no true skeletal retrusion exists = manage as soft tissue lower lid deformity.
If skeletal retrusion confirmed = proceed to Step 2.
Step 2: Evaluate Occlusion
Normal Occlusion
- Class I relationship
- No functional malocclusion
- No maxillary retrusion affecting bite
? Implant-based reconstruction preferred.
Abnormal Occlusion
- Class III tendency
- Maxillary hypoplasia
- Functional malocclusion
- Orthognathic consultation required.
If occlusion drives deformity, skeletal repositioning may be indicated.
Step 3: Assess Severity of Skeletal Retrusion
Mild (1–2 mm infraorbital retrusion)
- Minimal scleral show
- Tear trough dominant
Management:
- Consider infraorbital-only or smaller infraorbital-malar custom implant
- Soft tissue adjuncts as needed
 Consider infraorbital-only or smaller infraorbital-malar custom implant
Consider infraorbital-only or smaller infraorbital-malar custom implantModerate (2–5 mm retrusion)
- Visible negative vector
- Paranasal depression
- Tear trough + lid-cheek junction disruption
Management:
- Infraorbital–maxillary implant
- Custom design with zonal transition
- Screw fixation recommended
 Infraorbital–maxillary implant
Infraorbital–maxillary implantSevere (>5 mm retrusion)
- Marked scleral show
- Global midface flatness
- Malar deficiency
- Possible occlusal involvement
Management:
- Combined infraorbital–malar–maxillary “midface mask” implant
OR - Orthognathic advancement (if occlusal component present)
OR - Combined orthognathic + implant refinement
 Combined infraorbital–malar–maxillary “midface mask” implant
Combined infraorbital–malar–maxillary “midface mask” implantStep 4: Evaluate Lower Eyelid Stability
Good Lid Tone
- Normal snap test
- No significant laxity
– Skeletal augmentation alone may suffice.
Mild Laxity
- Borderline snap test
- Mild scleral show
– Skeletal augmentation + canthopexy.
Significant Laxity
- Positive distraction test
- Ectropion tendency
- Canthoplasty required in addition to skeletal correction.
Important Principle:
Lower eyelid surgery alone will not correct skeletal negative vector.
Step 5: Assess Soft Tissue Envelope
Thick Skin / Adequate SOOF
- More forgiving projection
- Standard zonal transitions acceptable
Thin Skin / Minimal Soft Tissue
- High visibility risk
- Requires:
- Conservative projection
- Extended feathered edges
- Avoid infraorbital overbuilding
In thin-skinned patients, even 1 mm overprojection may be visible.
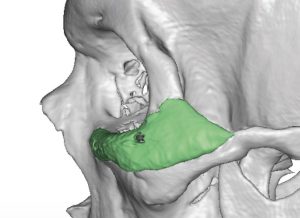
Step 6: Determine Implant Design Strategy
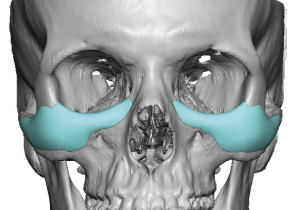
A. Infraorbital-Only Implant
 Indicated when:
Indicated when:
- Isolated rim retrusion
- Minimal paranasal concavity
- Adequate malar projection
Projection Range:
2–3 mm typical
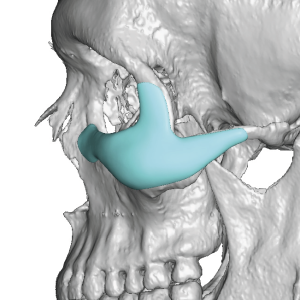
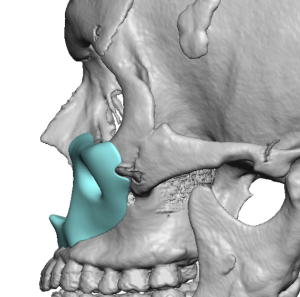
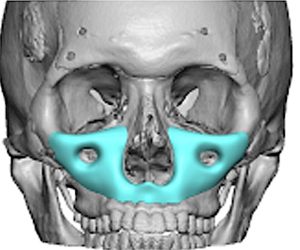
B. Infraorbital–Maxillary Implant
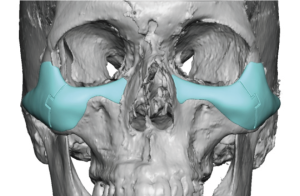
 Indicated when:
Indicated when:
- Tear trough + paranasal depression
- Central midface flatness
- Moderate negative vector
Projection Range:
- Infraorbital: 2–3 mm
- Maxilla: 4–6 mm
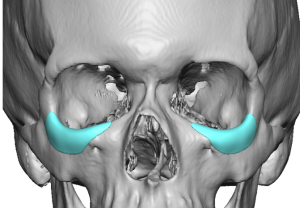
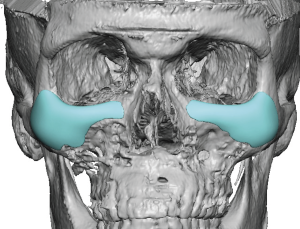
C. Midface Mask Implant
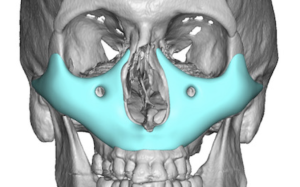 Indicated when:
Indicated when:
- Combined infraorbital, paranasal, and malar deficiency
- Severe negative vector
- Global flatness
Requires:
- Continuous topographic design
- 2–3 fixation points per side
Step 7: Consider Adjunctive Procedures
May Be Combined With:
- Lower eyelid spacer graft
- Fat repositioning
- Subperiosteal midface lift
Should Not Be Used Alone:
- Fillers (temporary)
- Fat grafting in severe skeletal deficiency
Soft tissue augmentation cannot structurally correct negative vector.
Decision Tree Summary
1. Confirm skeletal retrusion
- 3D CT scan
2. Evaluate occlusion
Normal = Implant pathway
Abnormal = Orthognathic evaluation
3. Grade severity
Mild = Infraorbital implant
Moderate = Infraorbital–maxillary implant
Severe = Midface mask ± orthognathic
4. Assess lid stability
Add canthopexy/canthoplasty if needed
5. Adjust projection based on soft tissue thickness
Key Biomechanical Principles
- Negative vector is a skeletal problem first.
- Lower eyelid surgery without skeletal support risks failure.
- Overcorrection produces artificial convexity.
- Projection should restore harmony, not create prominence.
- The infraorbital rim must transition smoothly into the maxilla and malar.
Common Errors in Management
- Treating tear trough with fillers alone in severe retrusion
- Performing blepharoplasty without correcting skeletal support
- Overbuilding infraorbital rim creating shelf deformity
- Ignoring paranasal depression
- Failing to evaluate occlusion
Conclusion
Management of negative vector midface requires structured analysis rather than isolated aesthetic intervention.
Proper sequencing includes:
- Confirming skeletal deficiency
- Evaluating occlusion
- Grading severity
- Assessing lid stability
- Designing zonal implant architecture
When correctly applied, implant-based reconstruction provides precise, predictable correction without altering occlusion. Orthognathic surgery remains indicated when functional malocclusion drives the deformity.
The most successful outcomes restore structural balance without visible signs of augmentation.
Dr. Barry Eppley
Plastic Surgery