

The nose is often perceived as a static structure on the face. But this is really only true for the upper part of the nose which is solid fixed bone. The bottom third, or the tip, is unfixed cartilage that can be easily moved. One of the ways it can move is through muscle action.
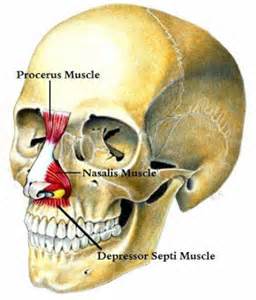 The depressor septi muscle is the one muscle that pulls on the tip of the nose. It is a paired very small muscle which is found one either side of the septum. It arises from the incisive fossa of the maxilla and ascends to insert into the nasal septum and the back part of the nasalis muscle. When it contracts it pulls the tip of the nose down and pulls upon the upper lip shortening it.
The depressor septi muscle is the one muscle that pulls on the tip of the nose. It is a paired very small muscle which is found one either side of the septum. It arises from the incisive fossa of the maxilla and ascends to insert into the nasal septum and the back part of the nasalis muscle. When it contracts it pulls the tip of the nose down and pulls upon the upper lip shortening it.
When the depressor septi nasi muscle is overactive, it creates the classic smiling deformity. This is seen as the nasal tip being pulled down, the upper lip shortening and, in some cases, a upper lip horizontal lip crease/wrinkle when one smiles. The smiling deformity is often treated concurrently during rhinoplasty to augment any tip changes after surgery or can be treated as an isolated procedure.
The surgical techniques for resecting an overactive depressor septi nasi muscle vary. In the February 2014 issue of Plastic and Reconstructive Surgery a study appeared entitled ‘Smile Analysis in Rhinoplasty: A Randomized Study for Comparing Resection and Transposition of the Depressor Septi Nasi Muscle’. In this paper two techniques (intranasal resection and intraoral transposition) of depressor septi nasi muscle treatment were performed randomly in rhinoplasty surgery in in 100 consecutive cases. Before and after surgery smile analysis and nasal measurements were done. Before surgery, tip projection and and upper lip height were decreased with smiling. After surgery, these muscular effects on smiling were significantly decreased. The intranasal and intraoral techniques for muscle resection did not differ in how much they decreased the effects of smiling on the length of the nose, tip projection or upper lip height.
The traction effects of the depressor septi nasi muscle on the tip of the nose when smiling is well known and has been treated by a variety of techniques for decades. The intranasal approach is historically more common due to the anatomic location of the muscle when doing a closed rhinoplasty. It has a side benefit of decreasing the interalar distance. The intraoral approach has been more recently described undoubtably due to the now widespread use of open rhinoplasty. Coming from below (inside the mouth) allows an actual release and transposition of the paired muscles. This results in an increased fullness to the upper lip afterwards.
With either method, however, hyperactive depressor septi muscle surgery can be effective if a decrease in tip projection, upper lip height or a horizontal upper lip line occurs when smiling that creates an unattractive effect.
Dr. Barry Eppley
Indianapolis, Indiana