

There are many anatomic components that influence the shape of the eye. One of the most significant and commonly modified is that of the outer corner of the eye. The well known procedures of canthopexy and canthoplasty are widely used although there is frequent patient confusion as to the difference between them. At their most basic level a canthopexy is a more limited procedure that manipulates the tendon but maintains its attachment to the bone to produce some lower eyelid tightening. A canthoplasty more significantly changes the outer corner of the eye by moving the bony attachment of the tendon to a higher position along the rim, raising the outer corner of the eye.
 In Volume 39 of the 2019 issue of Aesthetic Surgery Journal an article was published entitled “Dynamic Canthopexy” Drill Hole Canthal Repositioning’. In this paper the authors describe what would be considered a reliable and standard technique for lateral canthoplasty, a double hole lateral orbital rim canthal repositioning technique done through an upper eyelid incision. Athough it is called a canthopexy procedure it is really a canthoplasty technique.
In Volume 39 of the 2019 issue of Aesthetic Surgery Journal an article was published entitled “Dynamic Canthopexy” Drill Hole Canthal Repositioning’. In this paper the authors describe what would be considered a reliable and standard technique for lateral canthoplasty, a double hole lateral orbital rim canthal repositioning technique done through an upper eyelid incision. Athough it is called a canthopexy procedure it is really a canthoplasty technique.
In thirty (30) patients over a ten year period this type of canthoplasty was performed for either a congenitally downward sloped palpebral fissure (18) or in patients with normal eyes who wanted a more upwardly sloped palpebral fissure. (12) Average operative time was one hour. All patients achieved good results with emphasis on the need for over correction and the patient’s willingness to accept the over corrected look until it settled. (which they all do) All results at six months after the procedure would be considered permanent. No significant complications occurred.
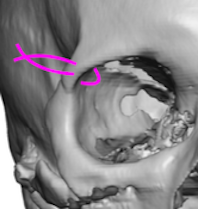
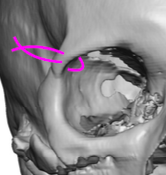
 The double hole lateral cantoplasty technique is the most assured method of significant lateral eye reshaping. The key is getting the drill holes up to or even above the frontozygomatic suture. It is possible to do so from the lower eyelid incision but coming from the upper eyelid approach assures the new lateral canthal position is not too low and keeps the lower eyelid incision small. The upper eyelid incision almost always heals inconspicuously.
The double hole lateral cantoplasty technique is the most assured method of significant lateral eye reshaping. The key is getting the drill holes up to or even above the frontozygomatic suture. It is possible to do so from the lower eyelid incision but coming from the upper eyelid approach assures the new lateral canthal position is not too low and keeps the lower eyelid incision small. The upper eyelid incision almost always heals inconspicuously.
Dr. Barry Eppley
Indianapolis, Indiana