


The length of the upper lip is an important and very changeable element of perioral aesthetics. Whether it is due to aging or naturally long upper lip it can be shortened by a variety of surgical excisional techniques of which the subnasal lip lift is the most well known and performed. While once regarded as a procedure avoided by plastic surgeons due to the resultant scar it is now commonly performed. And while many patients have so benefited from its increased use it is a procedure that should not be taken lightly despite its small size.
In the October 2023 issue of the journal Plastic and Reconstructive Surgery an article on this topic was published entitled ‘Lip Shortening Surgery’. In this paper the author reviews his experience with this aesthetic lip surgery based on 247 procedures (228 patients) over a 32 year practice period. The procedure is described as using a modified bullhorn incision at the base of the nose with accentuation for the eventual Cupid’s bow placement up into the introitus of the nose. The extent of the subnasal skin excision preserves 10mms of lip skin. This is done with the understanding that it is an irreversible procedure and a second stage lip lift is preferable to an upper lip that is too short. Some muscle division was done at the base of the nose. Closure was done at the dermis and skin layers but with no muscle sutures.
Of the 228 patients treated less than 1% were men. Almost 25% of the patients (53 or 23%) had a subsequent scar revision, most within the first 3 months of the surgery. Interestingly most of these scar revisions were performed by a hot-wire cautery for scar smoothing rather than excision. Secondary lip lifts were performed in 19 patients (8%), most within the first year of the first surgery.

 The most important element of this paper, and one that would only come from someone who has performed a lot of subnasal lip lifts, is that the scar is not to be underestimated in terms of potential visibility and that scar revisions are fairly common for it. Any area on the exposed lips and base of the nose is highly visible and patients will be very critical of how the scar looks. This should not be surprise and surgeons should be very accepting of it. As the author has discussed meticulous attention must be given to incisional placement, correction of asymmetries, and how the incision is closed, But even with the best of surgical technique scar revisions are not completely avoidable.
The most important element of this paper, and one that would only come from someone who has performed a lot of subnasal lip lifts, is that the scar is not to be underestimated in terms of potential visibility and that scar revisions are fairly common for it. Any area on the exposed lips and base of the nose is highly visible and patients will be very critical of how the scar looks. This should not be surprise and surgeons should be very accepting of it. As the author has discussed meticulous attention must be given to incisional placement, correction of asymmetries, and how the incision is closed, But even with the best of surgical technique scar revisions are not completely avoidable.

 Most of the author’s experience with the subnasal lip lift is in the older facial rejuvenation patient, which is understandable given that aging is a definitive cause of lip lengthening, and its incorporation into a more comprehensive facial rejuvenation surgery is a logical one. But the popularity of the procedure as well as the societal change in lip aesthetics has made the younger patient, with a naturally longer upper lip or even with a normal lip length, requesting the procedure. They may well want to violate the 10mm lip length preservation guideline, have tighter less aged tissues that may not scar as well and have an even higher critique of the subnasal scar and the aesthetic outcome than the older patient. As a result in a similar large number of younger patients (under 40 years of age) I would venture to predict the scar revision rate would be even higher than 25%.
Most of the author’s experience with the subnasal lip lift is in the older facial rejuvenation patient, which is understandable given that aging is a definitive cause of lip lengthening, and its incorporation into a more comprehensive facial rejuvenation surgery is a logical one. But the popularity of the procedure as well as the societal change in lip aesthetics has made the younger patient, with a naturally longer upper lip or even with a normal lip length, requesting the procedure. They may well want to violate the 10mm lip length preservation guideline, have tighter less aged tissues that may not scar as well and have an even higher critique of the subnasal scar and the aesthetic outcome than the older patient. As a result in a similar large number of younger patients (under 40 years of age) I would venture to predict the scar revision rate would be even higher than 25%.
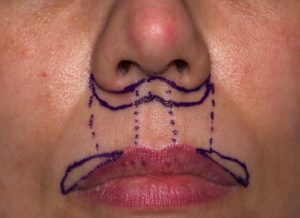

 The one element of the paper I found missing was the potential occurrence of an A-frame deformity due to residual inadequate lateral vermilion show. No matter how much the excision is extended up along the side of the nostril it can’t lift the thin or done turned outer third of the upper lip or mouth corner. For the sake of a more harmonious upper lip show in some patients adding a concurrent lateral vermilion advancement can offer an improved aesthetic result.
The one element of the paper I found missing was the potential occurrence of an A-frame deformity due to residual inadequate lateral vermilion show. No matter how much the excision is extended up along the side of the nostril it can’t lift the thin or done turned outer third of the upper lip or mouth corner. For the sake of a more harmonious upper lip show in some patients adding a concurrent lateral vermilion advancement can offer an improved aesthetic result.
Dr. Barry Eppley
World-Renowned Plastic Surgeon