

Introduction
Frontal bossing refers to a forehead shape in which the upper forehead protrudes farther forward than the lower brow area. This should be distinguished from the opposite condition, where the brow bones project more prominently than the upper forehead. Although both forms of forehead protrusion can occur in either gender, frontal bossing is more commonly seen in females, while excessive brow bone prominence is more typical in males.
Frontal bossing presents in a range of severities—from small, isolated bony prominences to large, convex upper foreheads. In its more pronounced aesthetic form, often accompanied by widening along the sides of the head, it can contribute to a macrocephalic appearance. This fronto-temporal widening is frequently associated with a high or elongated frontal hairline. While such head shapes may appear significant, they are typically normal developmental variations rather than signs of underlying pathology.
Aesthetic improvement of frontal bossing is achieved through bony reduction using burring or shaving of the frontal bone. In cases with fronto-temporal bossing, the bone reduction extends laterally toward the temporal bone, requiring contouring of the bony temporal line and sometimes partial removal or repositioning of the temporal muscle. The extent of achievable reduction depends on the thickness of the frontal bone, which must be evaluated preoperatively using a 3D CT scan.
Case Study
This young female patient presented with congenital frontal bossing and a broad head shape. Childhood photographs confirmed that the condition had been present since infancy. Her primary concern was the size and convexity of her forehead, though she was not bothered by her relatively high hairline.
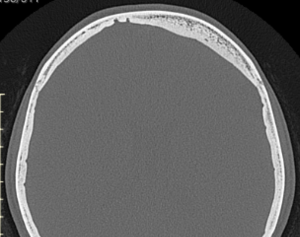
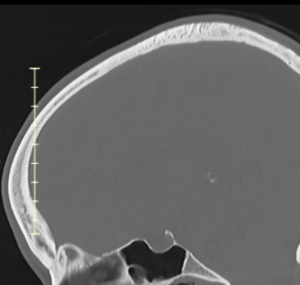 A 3D CT scan demonstrated sufficient frontal and temporal bone thickness to allow safe reduction.
A 3D CT scan demonstrated sufficient frontal and temporal bone thickness to allow safe reduction.

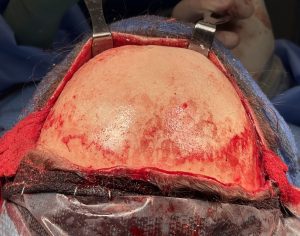 Under general anesthesia, a near-coronal scalp incision was made—without shaving or removing hair and sparing the lower temporal regions—to expose the entire forehead and upper temporal areas. Using a high-speed handpiece and burr, the frontal bossing was reduced by approximately 3–4 mm, down to just short of the diploic space, indicated by slight bone bleeding. On the thicker side, additional contouring was performed.
Under general anesthesia, a near-coronal scalp incision was made—without shaving or removing hair and sparing the lower temporal regions—to expose the entire forehead and upper temporal areas. Using a high-speed handpiece and burr, the frontal bossing was reduced by approximately 3–4 mm, down to just short of the diploic space, indicated by slight bone bleeding. On the thicker side, additional contouring was performed.
 The posterior temporal muscle was completely removed, and the anterior temporal muscle was released from the bony temporal line, shortened, and resuspended deeper in the temporal fossa using micro screws securing the fascia to bone.
The posterior temporal muscle was completely removed, and the anterior temporal muscle was released from the bony temporal line, shortened, and resuspended deeper in the temporal fossa using micro screws securing the fascia to bone.

 The scalp was then closed over bilateral drains using absorbable sutures. The immediate postoperative contour improvement was readily visible.
The scalp was then closed over bilateral drains using absorbable sutures. The immediate postoperative contour improvement was readily visible.



 At follow-up a few days later, after drain and dressing removal, a notable reduction in both the frontal bossing and lateral head width was evident, despite mild residual swelling.
At follow-up a few days later, after drain and dressing removal, a notable reduction in both the frontal bossing and lateral head width was evident, despite mild residual swelling.
Discussion
Frontal bossing with lateral head widening is congenitally determined and likely influenced by early brain growth patterns. It is not typically caused by excessive bone thickness; in fact, the bone may be thinner than average. Consequently, complete normalization of the forehead contour is rarely achievable, as the degree of reduction is limited by bone thickness—particularly over the upper forehead and along the temporal lines.
However, meaningful aesthetic improvement can be achieved through combined bone and muscle reduction. The posterior temporal muscle can be safely excised without functional compromise, and partial reduction of the anterior temporal muscle synergizes with bony contouring to effectively narrow the upper head shape.
A coronal incision provides the necessary exposure for such comprehensive reshaping. The incision, however, need not extend entirely to the ears; minimizing the temporal length improves scar quality. Hair shaving is unnecessary—meticulous incision design and closure techniques preserve hair follicles, allowing regrowth directly up to the scar line and minimizing visible scarring.
The goal of frontal bossing reduction is not to achieve a perfectly “flat” or normalized forehead, but to transform a conspicuously protruding or wide forehead into one that appears proportionate and natural within the normal aesthetic range.
Key Points
- Frontal bossing and head widening are congenital and can be improved through combined bone and muscle reduction, limited by skull bone thickness.
- Effective fronto-temporal contouring requires a near-coronal scalp incision for adequate access.
- The frontal bone in females is generally thin, limiting the extent of safe reduction achievable.
Barry Eppley, MD, DMD
World-Renowned Plastic Surgeon