

Abstract
Forehead augmentation is an established craniofacial aesthetic procedure used to alter contour, projection, and symmetry of the upper facial skeleton. Two primary structural methods are employed: intraoperatively sculpted bone cements and preoperatively designed custom implants. Although both techniques provide permanent augmentation, they differ significantly in fabrication method, precision of shape control, surgical requirements, and clinical indications. This article reviews and compares these approaches, highlighting their respective advantages, limitations, and optimal use cases.
Introduction
Aesthetic forehead augmentation addresses congenital or acquired flatness, concavity, asymmetry, or insufficient projection of the frontal bone. Historically, bone cements represented the sole option for structural forehead augmentation. Advances in three-dimensional imaging, computer-assisted design, and implant manufacturing have since introduced custom implants, allowing for greater control over forehead shape and volume. Understanding the distinctions between these two techniques is essential for appropriate patient selection and optimal aesthetic outcomes.
Materials and Methods
Bone Cement
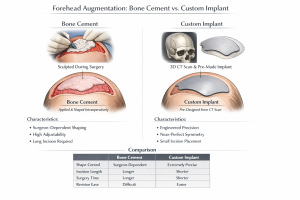
 Bone cement augmentation involves intraoperative hand sculpting of material directly onto the frontal bone. Commonly used materials include polymethylmethacrylate (PMMA) and hydroxyapatite (HA). The final shape is entirely dependent on the surgeon’s experience and technical skill, with adjustments made during surgery prior to material setting.
Bone cement augmentation involves intraoperative hand sculpting of material directly onto the frontal bone. Commonly used materials include polymethylmethacrylate (PMMA) and hydroxyapatite (HA). The final shape is entirely dependent on the surgeon’s experience and technical skill, with adjustments made during surgery prior to material setting.
Custom Implants
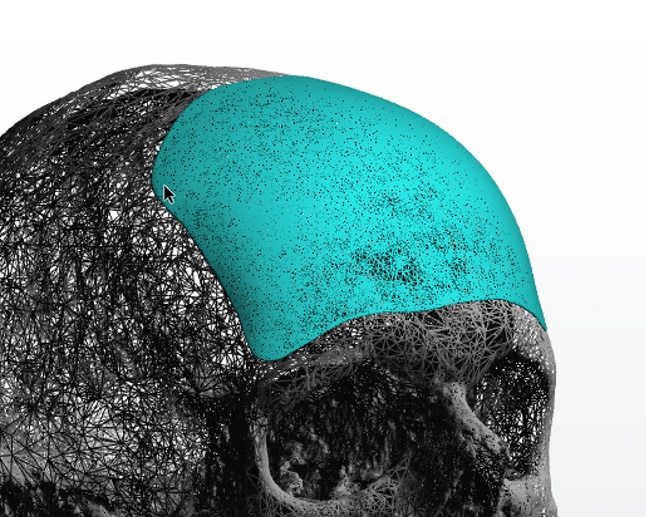
 Custom implants are designed preoperatively using high-resolution CT imaging. Computer-assisted design allows precise control over contour, thickness, symmetry, and edge transitions. Implants are manufactured prior to surgery and inserted as a preformed onlay during the operative procedure.
Custom implants are designed preoperatively using high-resolution CT imaging. Computer-assisted design allows precise control over contour, thickness, symmetry, and edge transitions. Implants are manufactured prior to surgery and inserted as a preformed onlay during the operative procedure.
Shape Control and Precision
Both techniques can achieve satisfactory aesthetic outcomes; however, the degree of predictability differs.
Bone cement allows real-time intraoperative modification but is inherently surgeon-dependent. Symmetry and contour accuracy are generally good but limited by manual sculpting. Custom implants provide near-perfect bilateral symmetry and precise replication of the planned design, with minimal intraoperative variability.
Indications
Bone cement is best suited for:
- Mild to moderate frontal flatness or concavity
- Subtle convex contouring, commonly desired in female patients
- Minor asymmetries
- Cases managed by surgeons experienced in craniofacial cement sculpting
Custom implants are best suited for:
- Significant congenital or structural forehead deficiency
- Posteriorly sloped or retrusive frontal bones
- Specific contour requirements, including brow ridge projection
- Large surface-area augmentation
- Cases requiring maximal symmetry and reproducibility
Surgical Considerations
 Bone cement placement typically requires a longer scalp incision and elevation of a forehead flap to allow adequate visualization and sculpting. While limited-access injection techniques exist, these are restricted to PMMA and are not applicable to HA materials.
Bone cement placement typically requires a longer scalp incision and elevation of a forehead flap to allow adequate visualization and sculpting. While limited-access injection techniques exist, these are restricted to PMMA and are not applicable to HA materials.
 Custom implants are generally inserted through smaller scalp incisions positioned posterior to the frontal hairline, reducing incision length and direct tissue manipulation.
Custom implants are generally inserted through smaller scalp incisions positioned posterior to the frontal hairline, reducing incision length and direct tissue manipulation.
Operative time is often longer for bone cement procedures due to sculpting requirements, whereas implant placement is more time-efficient once the implant is manufactured.
Recovery and Outcomes
Postoperative swelling and recovery timelines are similar for both techniques, with most patients resuming normal activities within 10–14 days. Final contour stabilization typically occurs by approximately three months postoperatively.
Risks and Limitations
Bone cement carries an increased risk of contour irregularities, asymmetry, and difficulty with revision or removal once fully integrated. Custom implants allow easier revision or replacement but require greater upfront planning, higher cost, and preoperative manufacturing time.
Discussion
 The evolution of forehead augmentation techniques reflects broader advances in craniofacial surgery. While bone cement remains a viable option for limited-volume, smooth contour augmentation, its indications are narrow due to constraints in predictable shape control and scalability. Custom implants offer unparalleled precision, reproducibility, and flexibility, making them the preferred method for complex or high-volume augmentations, particularly in male patients.
The evolution of forehead augmentation techniques reflects broader advances in craniofacial surgery. While bone cement remains a viable option for limited-volume, smooth contour augmentation, its indications are narrow due to constraints in predictable shape control and scalability. Custom implants offer unparalleled precision, reproducibility, and flexibility, making them the preferred method for complex or high-volume augmentations, particularly in male patients.
A common misconception is that bone cement represents a more “natural” augmentation due to presumed osseous integration. In craniofacial applications, PMMA functions as an onlay implant rather than a biologically integrating material, forming a fibrous interface with bone. Thus, its classification as “bone cement” is a historical artifact derived from orthopedic usage rather than a reflection of cranial biology.
This does differ from hydroxyapatite bone cement (HAC) in which bone does bond directly to the synthetic material. But HAC has more difficult handling and shaping properties, requires a far more open scalp incision, does not set well if the recipient site is not very dry and has high costs associated with it.
Conclusion
 Bone cement and custom implants are both effective tools for aesthetic forehead augmentation; however, their roles are distinctly different. Bone cement is best reserved for small-volume, smoothly contoured augmentations, while custom implants provide comprehensive control over shape, symmetry, and volume. Contemporary practice increasingly favors custom implant technology due to its predictability and expanded aesthetic capabilities.
Bone cement and custom implants are both effective tools for aesthetic forehead augmentation; however, their roles are distinctly different. Bone cement is best reserved for small-volume, smoothly contoured augmentations, while custom implants provide comprehensive control over shape, symmetry, and volume. Contemporary practice increasingly favors custom implant technology due to its predictability and expanded aesthetic capabilities.
Dr. Barry Eppley
World-Renowned Plastic Surgeon