

The desire for forehead reshaping in adults is done for three reasons. Most commonly, it is someone who has a residual forehead deformity due a congenital skull deformity. (e.g., craniosynostosis) As one gets older, or as hair loss occurs in men, the frontal skull deformity becomes more aesthetically obvious. Secondly, a frontal skull deformity exists due to an injury or after a neurosurgical craniotomy procedure has been done. Lastly, for those individuals going through a gender transition (female to male), the slope of the forehead or the prominence of the brows may be desired to be increased.
For any of these reasons, forehead augmentation (frontal cranioplasty) involves expansion of the existing bone boundaries. It is not practical to try and do this by manipulating the skull bone in most cases, as there is an easier and more effective solution…..build up the bone with synthetic materials. While I always try to avoid synthetic materials when it is possible, their use in forehead augmentation is the only practical and reasonable option in the vast majority of cases. (onlay cranioplasty) As such, a good working knowledge of the available synthetic materials for the skull is important.
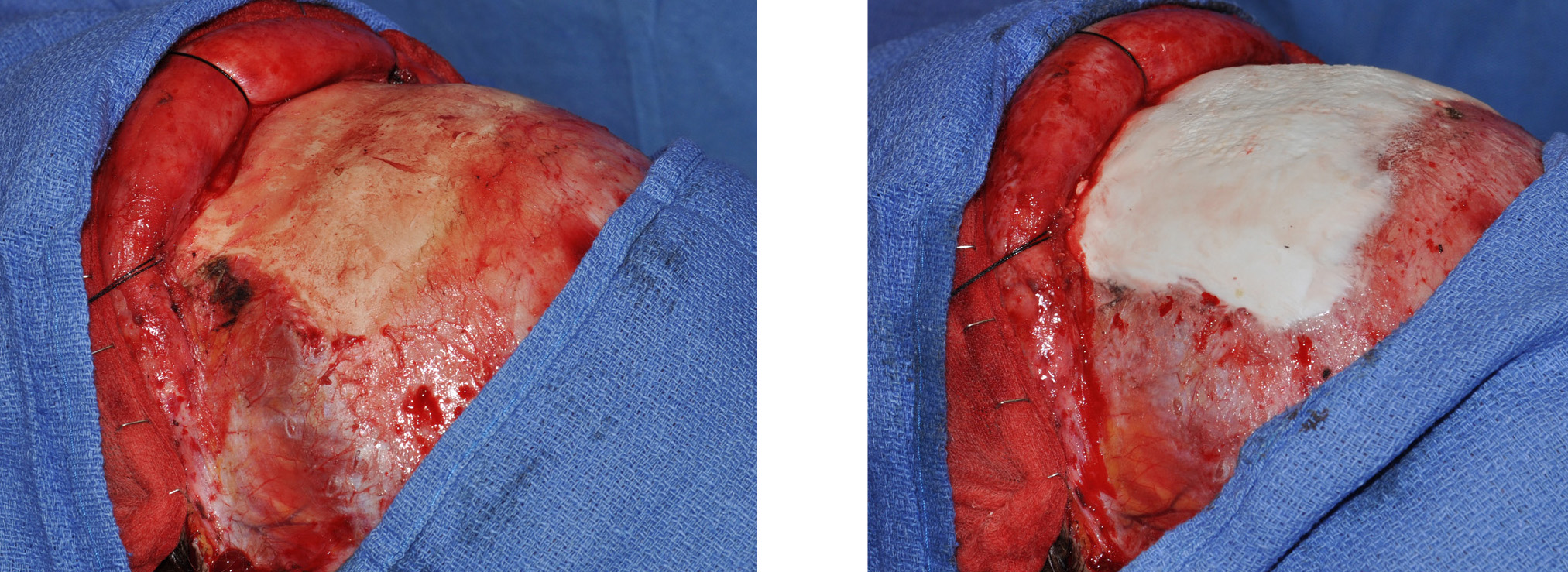 Fortunately, adding to the forehead bone is not a technically difficult procedure. The two questions about it are: what type of material to use…and access to the bone. Forehead augmentation has two very moldable and adaptable materials to build it up with. Traditional PMMA (polymethylmethacrylate) has been around for a long time and has the advantages of a very low cost, high resistance to impact forces, and ease of intraoperative contouring. Its main disadvantage is that some patients over time can develop some low-grade reactions to it and it may get loose, become infected or the overlying forehead skin may thin, although these issues are uncommon. It does generate a lot of heat during its setup (polymerization) but this is managed by cool water irrigation. Newer ‘more natural’ materials such as hydroxyapatite cements (HA) have been available over the past 10 years. HA offers the advantage of being a more natural, less synthetic material as its structure more closely resembles that of bone. Its disadvantages are that it is considerably more expensive, has a low resistance to impact (easily shatters), and is a bit tricker for the plastic surgeon to use. It generates no heat during its setup but is very sensitive to moisture and is easily deformed and pushed around during its set up phase. At this time, there are no long-term clinical studies that give a decided advantage to one material or the other.
Fortunately, adding to the forehead bone is not a technically difficult procedure. The two questions about it are: what type of material to use…and access to the bone. Forehead augmentation has two very moldable and adaptable materials to build it up with. Traditional PMMA (polymethylmethacrylate) has been around for a long time and has the advantages of a very low cost, high resistance to impact forces, and ease of intraoperative contouring. Its main disadvantage is that some patients over time can develop some low-grade reactions to it and it may get loose, become infected or the overlying forehead skin may thin, although these issues are uncommon. It does generate a lot of heat during its setup (polymerization) but this is managed by cool water irrigation. Newer ‘more natural’ materials such as hydroxyapatite cements (HA) have been available over the past 10 years. HA offers the advantage of being a more natural, less synthetic material as its structure more closely resembles that of bone. Its disadvantages are that it is considerably more expensive, has a low resistance to impact (easily shatters), and is a bit tricker for the plastic surgeon to use. It generates no heat during its setup but is very sensitive to moisture and is easily deformed and pushed around during its set up phase. At this time, there are no long-term clinical studies that give a decided advantage to one material or the other.
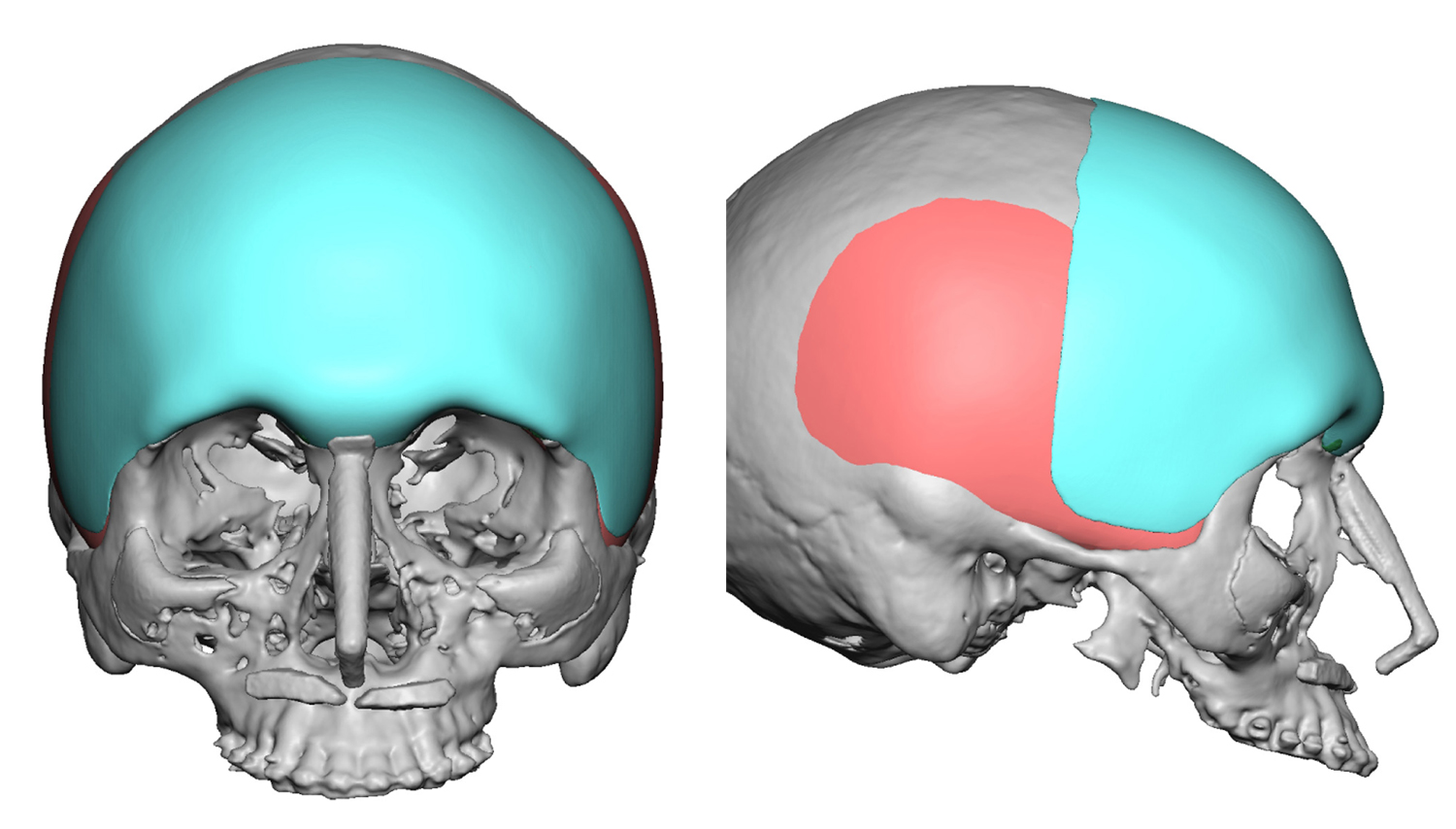 Other synthetic options include pre-made or custom-made synthetic implants. They can be made of either silicone rubber (most common), gore-tex, or poplyethylene. In most cases, these would have to be prefabricated based on a skull model of the patient to get the best and most exacting fit. Any irrergularities will be obvious in the contour of the forehead so a precision fit is essential. I don’t find that these onlay custom implants offer any advantages over PMMA or HA in terms of better long-term outcomes or reduced risks of complications.
Other synthetic options include pre-made or custom-made synthetic implants. They can be made of either silicone rubber (most common), gore-tex, or poplyethylene. In most cases, these would have to be prefabricated based on a skull model of the patient to get the best and most exacting fit. Any irrergularities will be obvious in the contour of the forehead so a precision fit is essential. I don’t find that these onlay custom implants offer any advantages over PMMA or HA in terms of better long-term outcomes or reduced risks of complications.
Regardless of the material used, synthetic forehead augmentation is all about access. The asiest and most predictable way to place it is through an open scalp incision. While this is the best and easiest way to do, there is always the cosmetic trade-off of this scar. When more limited or endoscopic access methods are used, one has to use PMMA because it is easier to mold through intact skin and will predictably stay where it is placed and molded. Endoscopic forehead augmentation is a more limited procedure due to its more limited visual access.
Dr. Barry Eppley
Indianapolis, Indiana