

While brow bone reduction is fairly well known because of the emergence of facial feminization surgery, less is known about its opposite cousin brow bone augmentation. While aesthetic brow bone augmentation has been done sporadically for years there has never been a completely satisfactory method for doing so. Different biomaterials have been used, usually hand crafted, and the method of placement of the implant has been through larger scalp incisions. All of these do not bode well for a predictable and significant brow bone augmentation effect.
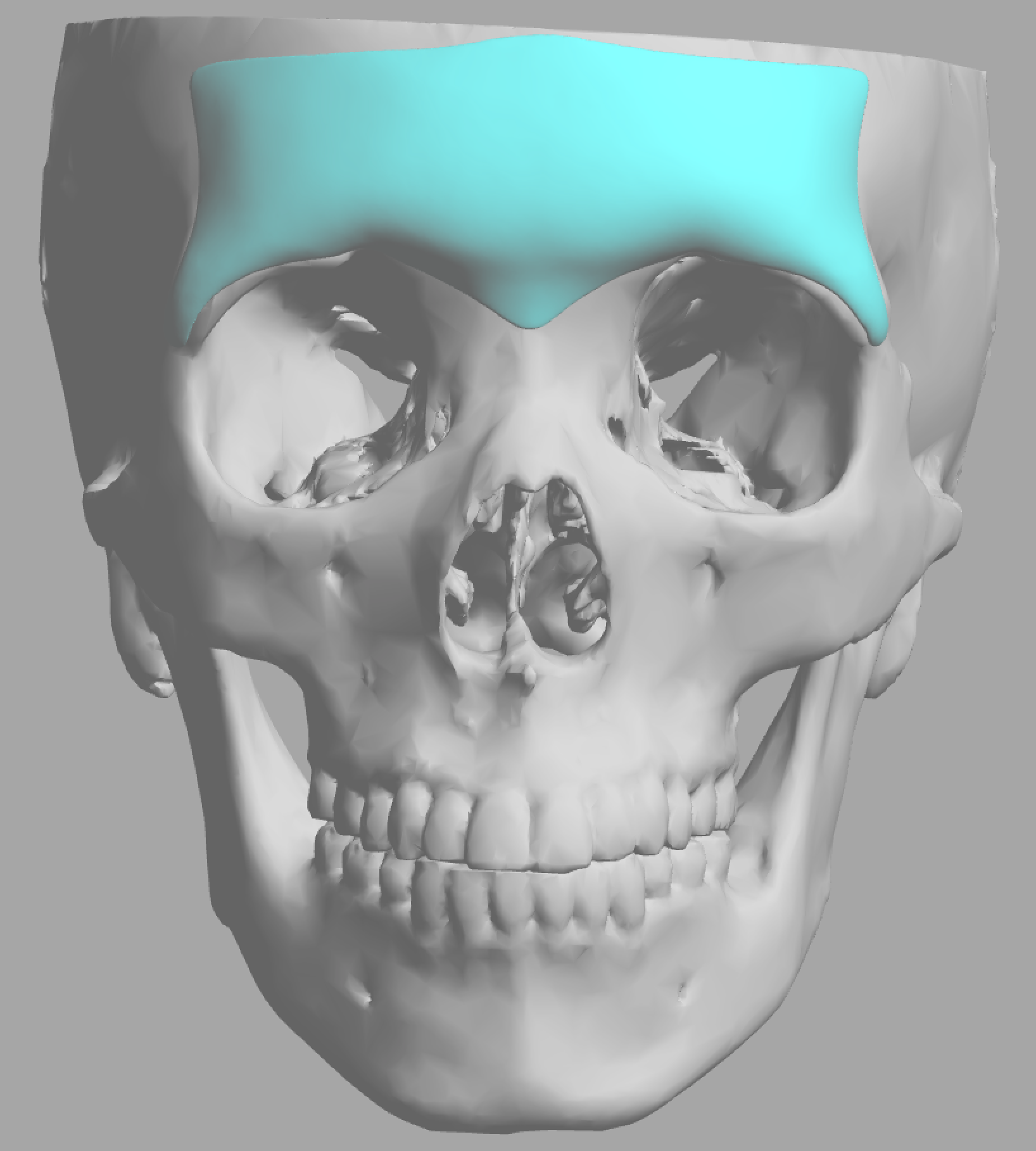
All that has changed in the past decade with the introduction custom facial implant technology. With this approach performed implants can be designed and manufactured from the patient’s 3D CT scan for their specific aesthetic needs. This is of particular relevance when it comes to the complex shape of the brow bone area and the need to place the implant with the lest amount of scarring as possible. (endoscopic technique)
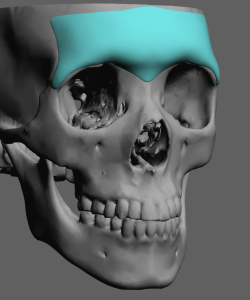
 While more men than women request brow bone augmentation, there are differences in their shapes that are important to incorporate into their designs. The male brow bone has four distinct mounds or projections that are separated centrally by a vertical glabellar valley. The inner bony mounds are created by a prominent frontal sinus development and is larger than the outer or more lateral bony mound. The smaller outer bony mound, which is composed of solid frontal bone) is more horizontally oriented as it eventually becomes the tail of the brow bone. While women have frontal sinuses they are much smaller and do not cause mound shaped protrusions. As a result their brow bones are ‘flatter’ with usually no distinction between the inner and outer mounds.
While more men than women request brow bone augmentation, there are differences in their shapes that are important to incorporate into their designs. The male brow bone has four distinct mounds or projections that are separated centrally by a vertical glabellar valley. The inner bony mounds are created by a prominent frontal sinus development and is larger than the outer or more lateral bony mound. The smaller outer bony mound, which is composed of solid frontal bone) is more horizontally oriented as it eventually becomes the tail of the brow bone. While women have frontal sinuses they are much smaller and do not cause mound shaped protrusions. As a result their brow bones are ‘flatter’ with usually no distinction between the inner and outer mounds.
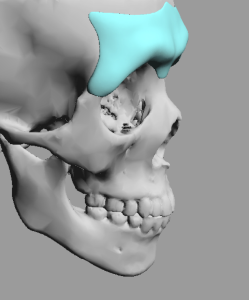
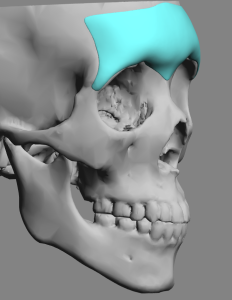 The larger mounds of the brow bones in men create a distinct and very visible suprabrow bone break as they transition up into the lower forehead. The smaller brow bones of females do not usually have any evidence of a suprabrow bone break and has a smooth transition superiorly into the forehead. This is particularly evident in profile.
The larger mounds of the brow bones in men create a distinct and very visible suprabrow bone break as they transition up into the lower forehead. The smaller brow bones of females do not usually have any evidence of a suprabrow bone break and has a smooth transition superiorly into the forehead. This is particularly evident in profile.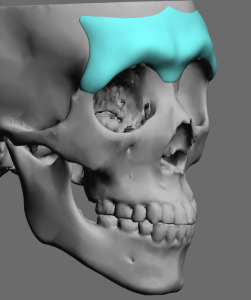
In the oblique view the male brow bone can appear to have a double bump due to the differences in the heights of the inner and outer mounds. Conversely in females there is little to no visible transition between the tail of the brow bone and the forehead.
While it is accepted that most male facial features are stronger or more pronounced than females, and the brow bones are no exception, there is more to it than just size. Men have a more complex topographic shape to their brow bones while women have a smaller more uniform shape. Such anatomic differences need to be built into custom brow bone implant designs to help maintain the augmented gender identity.
Dr. Barry Eppley
Indianapolis, Indiana