

Chin augmentation is one of the most common of all facial reshaping surgeries and is usually performed by the placement of an implant. This relatively ‘simple’ procedure works as long as the augmentation needs are within what the style and size of standard implants can provide.
But not all chin augmentation patients are accepting of a synthetic material in their face and some dimensional chin changes are beyond what a chin implant can achieve. This is where the role of a sliding genioplasty enters. This is the autologous chin augmentation surgery that can be a substitute for an implant. It also can provide more effective vertical chin lengthening and is the only chin procedure that can vertically shorten it. So either by choice or dimensional need the sliding genioplasty is chosen.
While there are numerous surgical debates about which chin augmentation procedure is best, these are really short sighted arguments. What matters is what can each dimensionally accomplish and, if it turns out they are similar to what the patient needs to achieve their goals, then the advantages and disadvantages of each can be discussed.
There are also situations where both methods of chin augmentation fall short. The amount of horizontal increase or vertical lengthening are beyond what the manufacturers have available as standard implant dimensions. There is also cases where the sliding genioplasty may not be able to be moved far enough forward due to the thickness of the bone or the downward or upward angulation of the osteotomy is done at the cost of an adequate amount of horizontal projection.
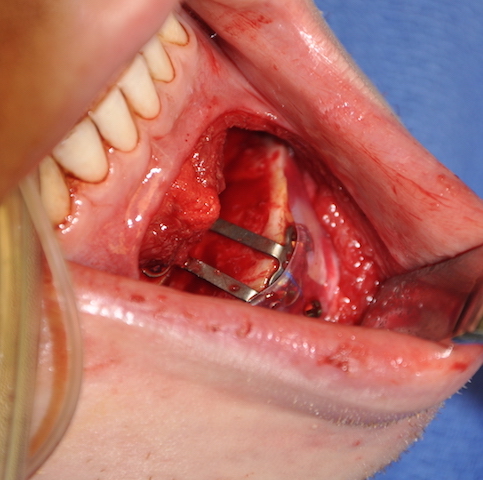
In these patients a sliding genioplasty and an implant can be combined in a dual chin augmentation technique. The sliding genioplasty serves as the foundation of the chin augmentation and creates the majority of the effect. The chin implant is added to it an an overlay to provide some extra horizontal increase and /or have its lateral extensions used to cover over the bony step offs at the back end of the osteotomy lines at the inferior border. Such implants need to be secured with screws to prevent an inevitable upward migration into the genioplasty step off if they are not.

 While many see chin bone movements and the use of implants as mutually exclusive they are not. The benefits of both procedures can be combined when the dimensional needs so dictate. Having done these chin augmentation combination many times over the years I see no increased risk of infection or problems with bone healing. Nor would I expect that to occur. The implant is not placed into the osteotomy gap and is just positioned in the front edge of the chin bone as it would normally be placed has a genioplasty not be done.
While many see chin bone movements and the use of implants as mutually exclusive they are not. The benefits of both procedures can be combined when the dimensional needs so dictate. Having done these chin augmentation combination many times over the years I see no increased risk of infection or problems with bone healing. Nor would I expect that to occur. The implant is not placed into the osteotomy gap and is just positioned in the front edge of the chin bone as it would normally be placed has a genioplasty not be done.
For a maximal chin augmentation effect, in patients whose dimensional needs exceed the capability of either standard approach, a combined osteotomy-implant technique can achieve an extraordinary result.
Dr. Barry Eppley
Indianapolis, Indiana