

Labiomental fold reduction by fat grafting is an effective way to soften the deep crease between the lower lip and chin while preserving a natural look.
 What the labiomental fold is
What the labiomental fold is
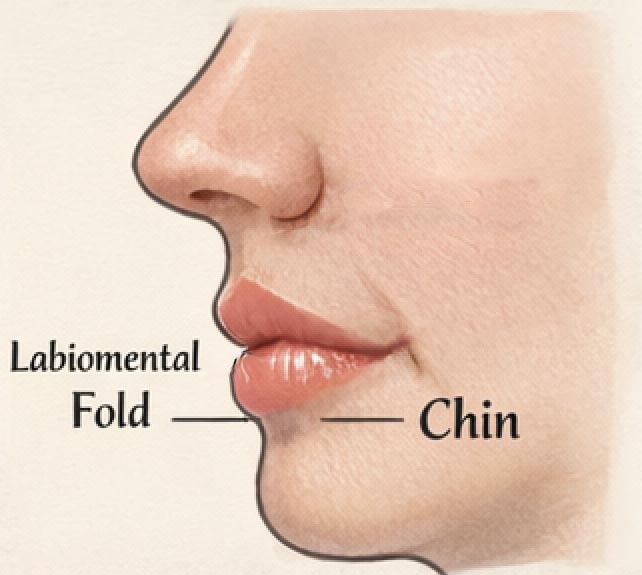
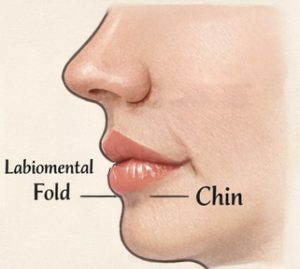
- The labiomental fold (mental crease) separates the lower lip from the chin pad
- It deepens with:
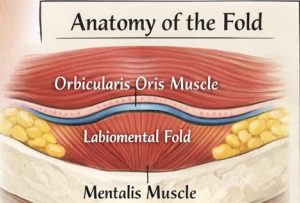
- Strong mentalis muscle activity
- Chin retrusion or vertical excess
- Chin augmentation of any form (implant or sliding genioplastyO
- Volume loss in the premental sulcus
- Aging-related soft-tissue descent
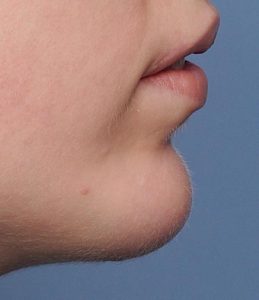
A very deep fold can make the chin look disconnected from the lower lip and create a “witch’s chin” or “pouting” appearance.
Fast grafting options
Fat grafting addresses the structural volume deficiency under the fold. It can be done by either an injection or a gram technique, each worth their own advantages.
Fat injection Technique
- Deep subcutaneous or supraperiosteal
- Avoid superficial placement ? visible lumpiness or contour irregularities
- Usual small volume amounts: 1–3 cc per side
- 0.7–1.2 mm blunt cannula preferred
- Short strokes, fan-like distribution
- Blend into the lateral labiomental region rather than focal filling
- Fat works best when structural support is adequate.
Ideal candidate
- Deep but soft labiomental fold
- Mild-to-moderate volume deficiency
- Stable chin projection
- Patient wants natural long-term improvement
Dermal Fat Graft instead of Fat injections
The labiomental fold is a high-motion, high-stress zone (mentalis + orbicularis oris). This leads to free (injected) fat propensities:
- Resorbs unpredictably
- Prone to migration
- Fails to resist dynamic crease formation
Dermal-fat graft advantages
- Dermis provides structural stiffness
- Better resistance to muscle animation
- Less resorption than pure fat
- Acts as a biologic “strut” across the fold
- More durable contour correction
This makes it ideal for deep, fixed, or recurrent folds.
Ideal indications
- Very deep labiomental crease
- Fold tethered to mentalis or dermis
- Failed fillers or prior fat grafting
- Revision cases
Donor site
Common choices:
- Lower abdomen (most common)
- Groin crease
- Prior incision sites (e.g., abdominoplasty scar)
 Graft thickness
Graft thickness
- Thin dermis with 3 – 5mm attached fat thickness (superficial plane)
- Thin dermis with 1 to 1.5cm attached fat thickness (deep plane)
Graft design
- Shape: elongated oval or cigar
- Length: ~2.5–4 cm
- Width: 5–8 mm
- Tapered ends to blend smoothly
The goal is crease effacement, not chin augmentation.
Pocket preparation (critical step)
- Intraoral vestibular approach
- Create a precise, snug pocket
- Superficial plane or deep plane
- Deep subcutaneous superficial to mentalis muscle with fold release
- Have to undermine the fold
- Under the mentalis muscle above the periosteum (deep plane)
 Placement technique
Placement technique
- Insert graft horizontally across the fold
- Dermis side:
- Usually oriented superficial
- Ensure symmetric placement
- Avoid folding or twisting
- The graft may be secured in the pocket with sutures
 Closure & postoperative care
Closure & postoperative care
- Two layer closure with resorbable sutures
- Avoid biting off food for 10 days until incision adequately heals.
- Expect firmness for several weeks before softening
 Outcomes
Outcomes
- Long-lasting improvement
- Natural chin–lip transition
- Particularly effective in the treatment of prior chin surgery tightness and deep fold.
- Results often superior to repeat filler or fat alone
Dr Barry Eppley
Plastic Surgeon