

The labiomental fold is the natural indentation that exists between the lower lip and the chin. It resides about 1/3 of the vertical distance between the lip and chin and is present in almost everyone to some degree. While called a fold, it is not really a fold but an indentation that is reflective of the lower extent of the vestibule intraorally. It exists because this is the level of where the origin of the mentalis muscle is as it takes off from the bone surface. Some fibers of the muscle insert into the deep dermis of the chin pad. Since one of the functions of the mentalis muscle is as an elevator of the central lower lip, the indentation can be come deeper with expression.
Very deep labiomental folds are often associated with short lower facial heights. Conversely, increased lower facial heights have more shallow effaced folds. Patients with normal lower facial heights have variable labiomental fold shapes. The aesthetics of the labiomental fold should be considered in any chin procedure since bony movement of the chin or its onlay augmentation is well known to affect the fold shape.
Another surgical issue that can affect the labiomental fold is intraoral surgical access to the chin. This requires cutting through the bony attachment of the mentalis muscle and then reattaching it during the closure. While not usually causing a labiomental fold problem the first time, repeat surgical entry may cause excessive scar tissue or a mentalis muscle reattachment that is very tight. This can make the labiomental fold deeper and/or feel very tight/stiff.
 Treatment of the tight or deep labiomental fold requires release and placement of an interpositional graft. A tight or scarred down labiomental fold represents loss of normal tissue and/or its elasticity. Trying to alter the mentalis muscle is not going to make it more free or release the labiomental fold tightness. Labiomental fold release is done by going through the mucosa (usually the old incisional scar) down to the mentalis muscle. But the mentalis muscle is not cut through or completely released. In some cases the more superficial fibers of the muscle are released if that helps make a deeper pocket or better releases the overlying labiomental fold.
Treatment of the tight or deep labiomental fold requires release and placement of an interpositional graft. A tight or scarred down labiomental fold represents loss of normal tissue and/or its elasticity. Trying to alter the mentalis muscle is not going to make it more free or release the labiomental fold tightness. Labiomental fold release is done by going through the mucosa (usually the old incisional scar) down to the mentalis muscle. But the mentalis muscle is not cut through or completely released. In some cases the more superficial fibers of the muscle are released if that helps make a deeper pocket or better releases the overlying labiomental fold.
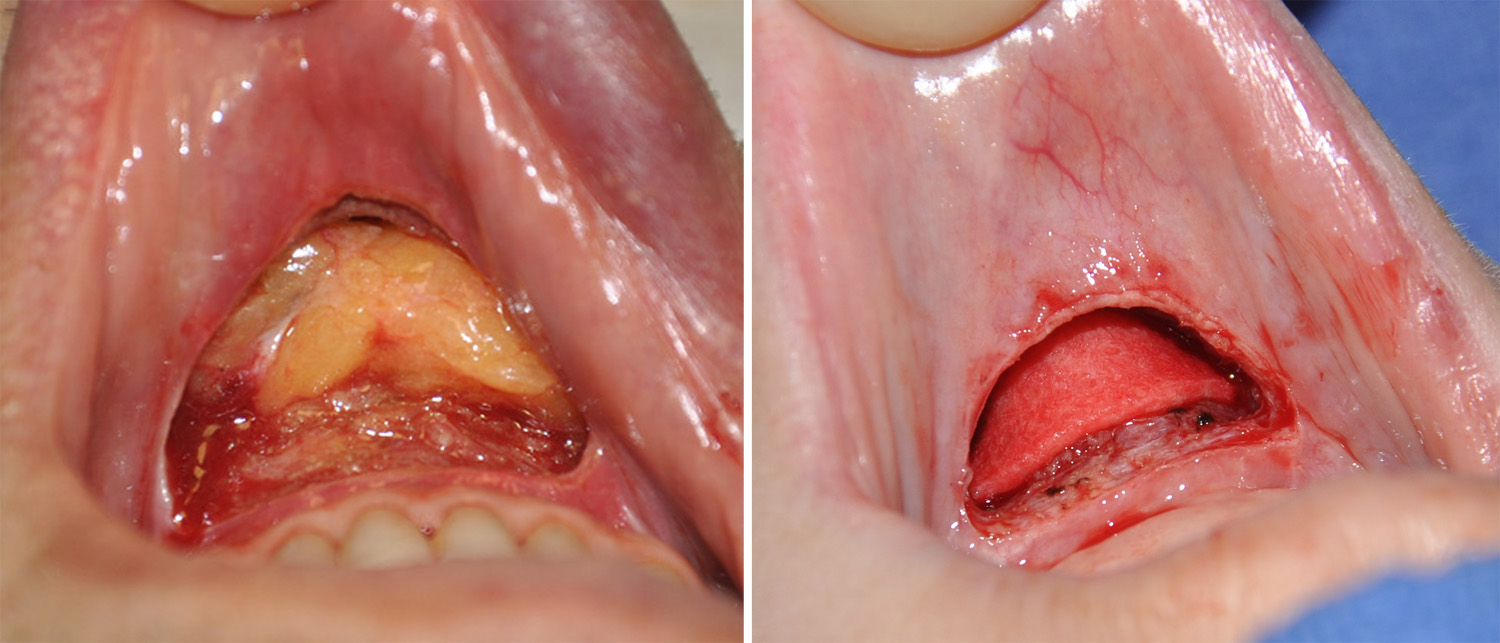 The interpositional graft placed beneath the labiomental fold can be of several material types. Choices include either cadaveric dermis material (e.g. Alloderm) or an autogenous dermal-fat graft. I favor the fat graft option since it is softer and provides more tissue volume. An injectable fat graft technique is an option but I don’t think it is an effective as actually opening the scarred area and applying a large fat graft into the open space.
The interpositional graft placed beneath the labiomental fold can be of several material types. Choices include either cadaveric dermis material (e.g. Alloderm) or an autogenous dermal-fat graft. I favor the fat graft option since it is softer and provides more tissue volume. An injectable fat graft technique is an option but I don’t think it is an effective as actually opening the scarred area and applying a large fat graft into the open space.
Most tight labiomental folds after chin surgery resolve over time. But if a tight and restrictive labiomental fold persists after 6 months or more of healing, release and tissue grafting is a treatment option.
Dr. Barry Eppley
Indianapolis, Indiana