

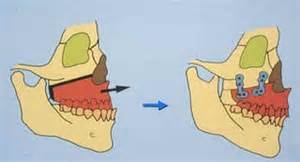
 The LeFort osteotomy is the well known of all facial osteotomies and is used to correct midface retrusion. In its most commonly used form, the LeFort I osteotomy, it is named after the fracture pattern originally described by Rene LeFort over one hundred years ago in that cuts are made across the maxilla above the tooth roots as well as through the pterygomaxillary junction. Although less commonly performed, higher levels of the LeFort osteotomy (II and III) are used for more complete midface deficiencies that are associated with craniofacial deformities.
The LeFort osteotomy is the well known of all facial osteotomies and is used to correct midface retrusion. In its most commonly used form, the LeFort I osteotomy, it is named after the fracture pattern originally described by Rene LeFort over one hundred years ago in that cuts are made across the maxilla above the tooth roots as well as through the pterygomaxillary junction. Although less commonly performed, higher levels of the LeFort osteotomy (II and III) are used for more complete midface deficiencies that are associated with craniofacial deformities.
Aesthetic midface deficiences are common in certain ethnic faces (e.g., Asian), traumatic midface fractures as well as general developmental patterns in some people. Many of these patients, however, can not be treated by LeFort osteotomies as they have a normal Class I or orthodontically corrected occlusion. Without the simultaneous correction of a malocclusion, the bone can not be brought forward otherwise it would create one. In addition, most aesthetic midface deficiencies do not justify skeletal correction due to the magnitude of the surgery and its associated risks.
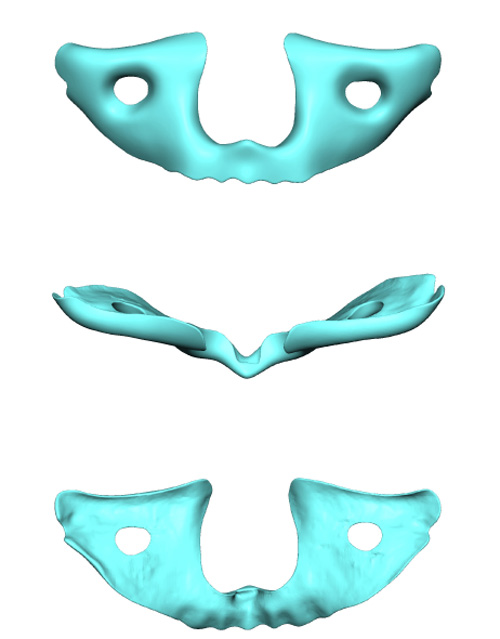 The custom midface implant offers an effective aesthetic operation that can have much of the same midface augmentation effect as many of the Lefort osteotomies. (minus the potential aesthetic benefit of forward teeth movement on the upper lip) It can cover the anterior face of the maxilla up onto the orbital rims and the cheeks. This can effectively pull the entire midface soft tissues forward including the base of the nose. It appears much like a mask in its design.
The custom midface implant offers an effective aesthetic operation that can have much of the same midface augmentation effect as many of the Lefort osteotomies. (minus the potential aesthetic benefit of forward teeth movement on the upper lip) It can cover the anterior face of the maxilla up onto the orbital rims and the cheeks. This can effectively pull the entire midface soft tissues forward including the base of the nose. It appears much like a mask in its design.
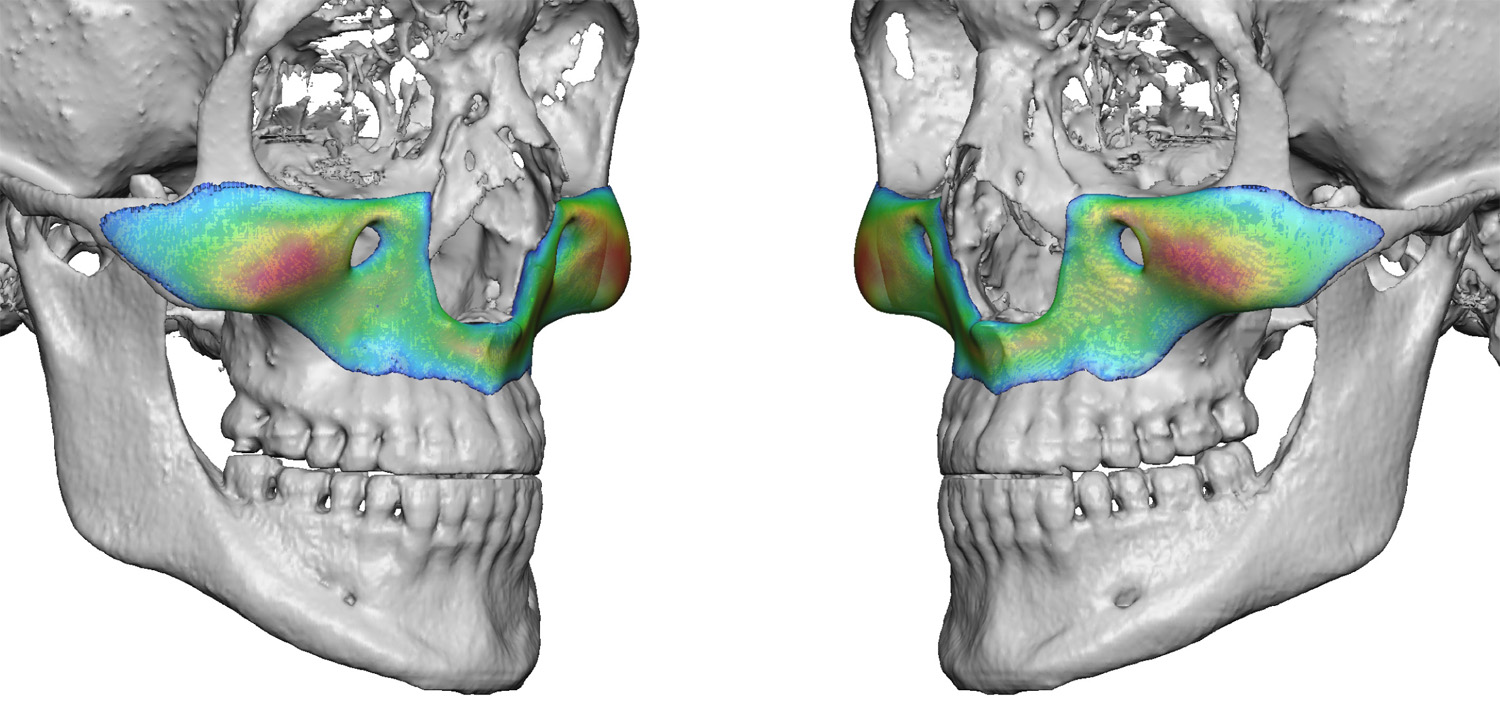 The design of the custom midface implant can done in variable amounts of dimensional changes across the face of the implant. The greatest fullness can be around the base of the nose and anterior nasal spine or it can be the exact opposite where it is thicker over the cheeks and infraorbital rim. It all depends on each patient’s aesthetic facial needs.
The design of the custom midface implant can done in variable amounts of dimensional changes across the face of the implant. The greatest fullness can be around the base of the nose and anterior nasal spine or it can be the exact opposite where it is thicker over the cheeks and infraorbital rim. It all depends on each patient’s aesthetic facial needs.
The custom midface implant is usually completely inserted from inside the mouth. In some cases where the implant comes ups around the infraorbital rims a lower eyelid incision may be needed to ensure its accurate positioning. The implant is inserted around the infraorbital nerve by making a slit in the implant above the nerve hole so it may safely wrap around it during insertion.
Dr. Barry Eppley
Indianapolis, Indiana