

One of most common forms of forehead reshaping surgery is augmentation of the brow ridges and frontal bone. Many more women than men historically undergo forehead augmentation surgery, most likely because of hairline and hair density issues. But some men still have the procedure as they value the improvement of their frontal skull/forehead shape as more important than the risk of an adverse scalp scar. Most commonly these men have a severe sloping inclination to their forehead in profile, an inclination that exceeds the more aesthetically acceptable inclination of 10 to 15 degrees and they may also lack significant brow ridge prominences.
 There are a variety of forehead augmentation materials that have been used, each with their own specific advantages and disadvantages. By far the most common material used historically is methylmethacrylate or PMMA. A self-curing plastic polymer, it is mixed during surgery as a liquid and powder and molded into shape and allowed to set. Its popularity is due its low associated cost in an area of craniofacial augmentation in which at least 30 or more grams of material is often needed. It is the easiest cranioplasty material to shape and becomes as hard as bone. Another material option is hydroxyapatite (HA), a synthetic ceramic material. It is also a liquid and powder composite like PMMA. But it has very different handling and set characteristics and good working experience is needed when using it as an onlay augmentation material. It is more sensitive to wetness and blood in the surgical site. But it is the ultimate biocompatible augmentation material because it is composed of the inorganic component of natural bone, calcium phosphate. Its high cost limits it use in large augmentations for many patients. ($100 per gram vs $10 per gram for PMMA)
There are a variety of forehead augmentation materials that have been used, each with their own specific advantages and disadvantages. By far the most common material used historically is methylmethacrylate or PMMA. A self-curing plastic polymer, it is mixed during surgery as a liquid and powder and molded into shape and allowed to set. Its popularity is due its low associated cost in an area of craniofacial augmentation in which at least 30 or more grams of material is often needed. It is the easiest cranioplasty material to shape and becomes as hard as bone. Another material option is hydroxyapatite (HA), a synthetic ceramic material. It is also a liquid and powder composite like PMMA. But it has very different handling and set characteristics and good working experience is needed when using it as an onlay augmentation material. It is more sensitive to wetness and blood in the surgical site. But it is the ultimate biocompatible augmentation material because it is composed of the inorganic component of natural bone, calcium phosphate. Its high cost limits it use in large augmentations for many patients. ($100 per gram vs $10 per gram for PMMA)
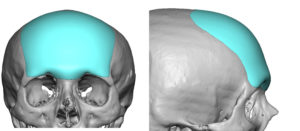
Regardless of the bone cement material used, it needs to be shaped to create the desired forehead shape. Besides the vertical inclination and the creation of a visible brow ridge if needed, the often overlooked part of forehead augmentation is its merging up to or across the anterior temporal line. A patient has to appreciate that you can not extend the bone cement material beyond the anterior temporal line which is the end of the width of the frontal bone. This is much more narrow that most people realize. Bone cements become unstable when placed onto the temporal fascia, particularly hydroxyapatite cements.
While traditionally a full open coronal incision is needed for optimal shaping of the material, this remains only true for the hydroxyapatite cements. If the forehead augmentation does not include the brow bones, it can done using PMMA through a far more limited scalp incision by an ‘injectable molding technique’. The working characteristics allow a subperiosteal tissue pocket to be created through which the PMMA material can be introduced and externally molded until set. There is a higher risk of potential material irregularities with this blinded technique and the user should have a lot of experience working with PMMA before attempting it. Any irregularities or asymmetries of the material is going to require a more extended scalp incision to adequately solve.
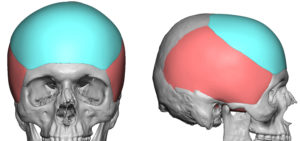
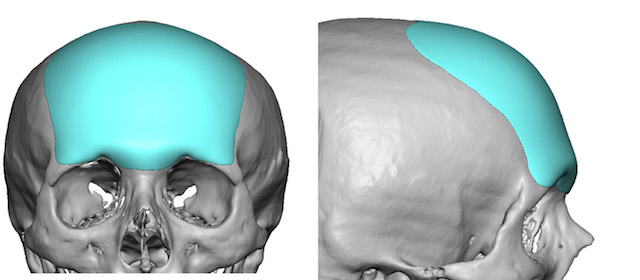
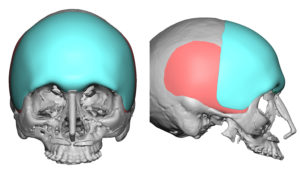 There are as of yet no preformed forehead augmentation implants available in the U.S. as an off-the-shelf choice. The best option, however, even if such preformed implants did exist is that of a custom forehead implant. This requires a 3-D CT scan of the patient from which a custom forehead implant is designed. This approach has many advantages and has almost completely replaced the use of bone cements in my practice. Its advantages include a specific fit for each patient and the capability to design every dimensional aspect of the implant to the patient’s specific aesthetic needs. Custom forehead implants also have the advantage that they can be extended beyond the temporal line and onto the softer temporalis fascia/muscle.
There are as of yet no preformed forehead augmentation implants available in the U.S. as an off-the-shelf choice. The best option, however, even if such preformed implants did exist is that of a custom forehead implant. This requires a 3-D CT scan of the patient from which a custom forehead implant is designed. This approach has many advantages and has almost completely replaced the use of bone cements in my practice. Its advantages include a specific fit for each patient and the capability to design every dimensional aspect of the implant to the patient’s specific aesthetic needs. Custom forehead implants also have the advantage that they can be extended beyond the temporal line and onto the softer temporalis fascia/muscle.
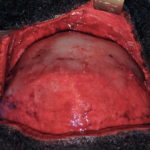
The use of custom implants for forehead augmentation has major implications in surgical placement and a resultant far smaller scalp scar needed. While several material options exist from which the implant can be made, solid silicone is the most economical and versatile material.
Dr. Barry Eppley
Indianapolis, Indiana