

Facial implants remain a good and simple way to highlight existing or deficient facial anatomy. While everyone knows the most common facial implants, such as cheeks and chins, there are numerous other areas of the face that can implanted.
In the midface, there are the standard implants of the cheeks and nose. These areas represent convex facial areas that are more commonly implanted because their lack of prominence is well recognized and aesthetically more obvious.
The midface also has areas of concavities that can benefit from bony augmentation. These areas are less well recognized because they are skeletal concavities. As such, the benefits of their expansion or augmentation are not as apparent.
These midfacial areas are known as the maxillary, premaxillary, and paranasal areas. To some degree, these three areas all run together and are contiguous. But they are separate implants for each area. They all address areas of flatness or excess concavity to the midfacial area.
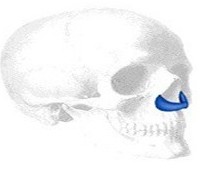 The paranasal implant addresses flatness underneath the base of the nose. This can occur from a congenital problem such as cleft lip and palate but most commonly is just the natural development of one’s face. The midface is flatter overall and one will frequently have cheek deficiencies as well. Most noticeable is that the nose is less pronounced and the base of the nose is positioned behind the projection of the upper front teeth in profile.
The paranasal implant addresses flatness underneath the base of the nose. This can occur from a congenital problem such as cleft lip and palate but most commonly is just the natural development of one’s face. The midface is flatter overall and one will frequently have cheek deficiencies as well. Most noticeable is that the nose is less pronounced and the base of the nose is positioned behind the projection of the upper front teeth in profile.
Premaxillary implants help bring out the entire base of the nose. They bring projection to the entire nasal base, most prominently the anterior nasal spine area. By using an implant across this area, the nasolabial angle is opened up by being brought forward. This can also give the illusion of increased nasal tip projection as well.
The maxillary implant is the least used facial implant of them all. It is really an extended paranasal implant which extends back along the maxilla above the roots of the upper teeth. It can also be used for paranasal or base of the nose augmentation but adds more fullness to the entire lower midface as well. Their effects are somewhat similar to what a LeFort I advancement osteotomy (2 to 4mms) may do.
Like all midface implants, they can be placed through an intraoral approach through a high vestibular incision. The periosteum needs to be elevated and the implants should be secured to the bone with screw fixation.
There are no definite methods of assessment that can determine the indications for these types of facial implants. Their use is based on an artistic or aesthetic sense of facial balance and the results can not be well predicted based on some form of computer analysis or prediction. In my Indianapolis plastic surgery practice, I find that their use is most commonly done with other facial procedures such as rhinoplasty, chin and cheek augmentation and mid- and lower facelifts.
Dr. Barry Eppley
Indianapolis, Indiana