

The mentalis is a well known muscle of the chin. Any chin surgery procedure involves manipulation of this muscle no matter what type of dimensional chin change is being done or how it is being done. (implant vs. osteotomy vs osteotomy) Since it is the only muscle that has attachments to the anterior surface of the chin bone, postoperative problems with its function can occur. While many chin procedures are done successfully with the return of normal muscle function, mentalis muscle dysfunction is not rare and is a frequent source of after surgery chin problems. Given the frequent misunderstanding of the mentalis muscle anatomy and function amongst patients and even some surgeons, its role and relevance in chin augmentation surgery merits review.
The mentalis is a paired central muscle of the chin that runs vertically over the chin bone. It actually has two halves and is separated by a fat pad that is most prominent near its bony origin underneath the labiomental fold below the lower lip. The relevance of this central fat pad in the muscle is not clear. The muscle is attached to the bone at the depth of the internal vestibule superiorly and runs down vertically to insert into the soft tissues of the lower submental chin pad. It is important to appreciate that the point of firm fixation is at its origin to the bone but its insertion is into the soft tissue inferiorly. The primary function of the muscle is contraction of the chin pad superiorly and inward (towards the lower lip) which will concurrently raise the lower lip creating a pout type facial expression. It is innervated by the marginal mandibular branch of the facial nerve which crosses over the jawline laterally to reach the muscle’s surface.
In chin augmentation surgery incisional access is either intraoral through the mucosa or submental through the skin. In sliding genioplasty the only choice is intraoral. But implant placement can be done both ways. Both incisional approaches cut through the mentalis muscle but they do so through different areas of the muscle. (origin or insertion. This is more than just an anatomic distinction, it can have a significant influence on muscle tension and function after surgery.
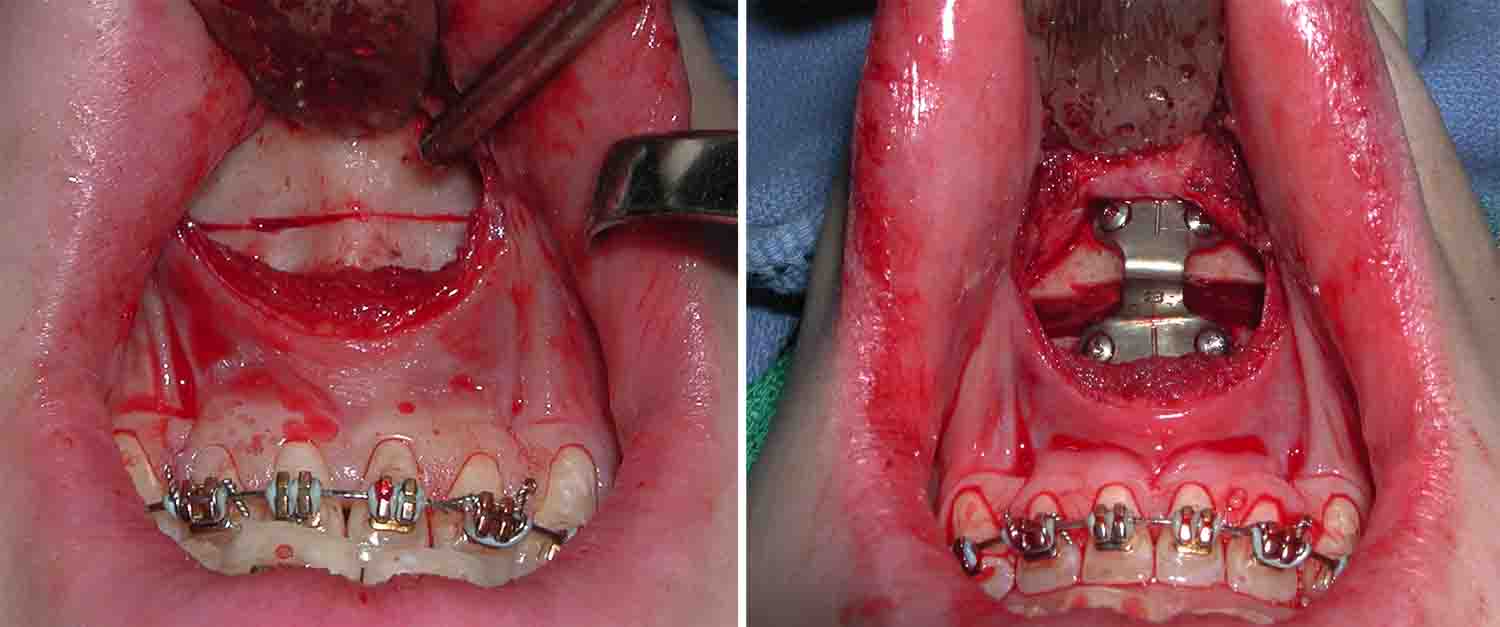 Cutting through the insertion of the muscle with an intraoral approach does so at the point of its maximal muscle thickness and tension. It is extremely important to leave an adequate cuff of muscle attached to the bone with this maneuver, otherwise there will be nowhere to attach the released inferior bulk of the muscle bellies. Without a reattachment the muscle will contract down, the labiomental fold will get deeper and the chin pad will pull down off of the bone. (chin ptosis)
Cutting through the insertion of the muscle with an intraoral approach does so at the point of its maximal muscle thickness and tension. It is extremely important to leave an adequate cuff of muscle attached to the bone with this maneuver, otherwise there will be nowhere to attach the released inferior bulk of the muscle bellies. Without a reattachment the muscle will contract down, the labiomental fold will get deeper and the chin pad will pull down off of the bone. (chin ptosis)
With a retained muscle cuff onto which the released muscle can be reattached, one is essentially re-establishing muscle length at the thickest part of the muscle. But it is easy to see how the muscle length is changed when the soft tissue chin pad is stretched out by an implant or an advanced bony chin segment. The larger the chin pad displacement the tighter the muscle closure will be. This accounts for many a patient’s complaints of prolonged chin tightness and stiffness after a sliding genioplasty, particularly in large advancements. It can also occur with chin implants and is most commonly seen when the implant rides up high and pressures the resutured muscle origin.
 In the submental approach for chin implants, it is the insertion of the muscle that must be cut and lifted up to reach the bone. Since this is not a firm bony attachment, muscle elevation and closure is done at the thinner lower portion of the muscle and has a much lower risk of adversely affecting muscle tension and postoperative function. This is why there are far fewer complaints of chin stiffness and tightness from submentally placed chin implants as re-establishing muscle length is much easier as opposed to pulling the muscle back up to its original bony attachment.
In the submental approach for chin implants, it is the insertion of the muscle that must be cut and lifted up to reach the bone. Since this is not a firm bony attachment, muscle elevation and closure is done at the thinner lower portion of the muscle and has a much lower risk of adversely affecting muscle tension and postoperative function. This is why there are far fewer complaints of chin stiffness and tightness from submentally placed chin implants as re-establishing muscle length is much easier as opposed to pulling the muscle back up to its original bony attachment.
 Mentalis muscle anatomy and its function is just one issue to consider in chin augmentation and is most relevant with implants where both incisional options are in play. When the patient prefers an intraoral approach for a standard chin implant I use the muscle splitting approach through its septum rather than cutting the muscle’s bony attachment.
Mentalis muscle anatomy and its function is just one issue to consider in chin augmentation and is most relevant with implants where both incisional options are in play. When the patient prefers an intraoral approach for a standard chin implant I use the muscle splitting approach through its septum rather than cutting the muscle’s bony attachment.
Dr. Barry Eppley
Indianapolis, Indiana