

Cheek implants are the third most commonly performed facial implant procedure. Trailing behind nasal and chin implants, cheek implants provide augmentation to a lateral facial structure and not a midline one. As a result most cheek augmentations are bilateral or paired and that poses a unique challenge in their surgical placement.
But prior to having them surgically placed is one of preoperative implant selection. While the cheek or zygomatic bone seems like a relatively simple convex structure, it actually has multiple aesthetic zones (malar, submalar, anterior infraorbital and posterior arch zones) that must be considered. Not every patient wants exactly the same area of the cheek augmented let alone be the same size. This helps to explain why there are so many different cheek implant styles from which to choose. From one manufacturer alone (Implantech) there are seven (7) different cheek implant style options.
While these current and commonly uses styles of cheek implants work for most patients, they are not aesthetically ideal for some patients and the facial change they hope to achieve. One type of cheek augmentation look for which standard cheek implants usually fail to achieve is that of the ‘high cheekbone’ look. This is also commonly referred to as the ‘model look’.
 Whether it be a man or women the model look refers to high cheekbones. These are cheeks that would be considered highly placed and robust. It is not that they as so big or protrude a lot to the sides. Rather their location and shape have the ability to add some angularity to the face by creating submalar hollows beneath the cheekbones. This is also a type of facial look which is not just located over the malar eminence but also creates a horizontal ridge along the entire length of the zygomatic process. Not such cheek implant style today can create that type of midface effect.
Whether it be a man or women the model look refers to high cheekbones. These are cheeks that would be considered highly placed and robust. It is not that they as so big or protrude a lot to the sides. Rather their location and shape have the ability to add some angularity to the face by creating submalar hollows beneath the cheekbones. This is also a type of facial look which is not just located over the malar eminence but also creates a horizontal ridge along the entire length of the zygomatic process. Not such cheek implant style today can create that type of midface effect.
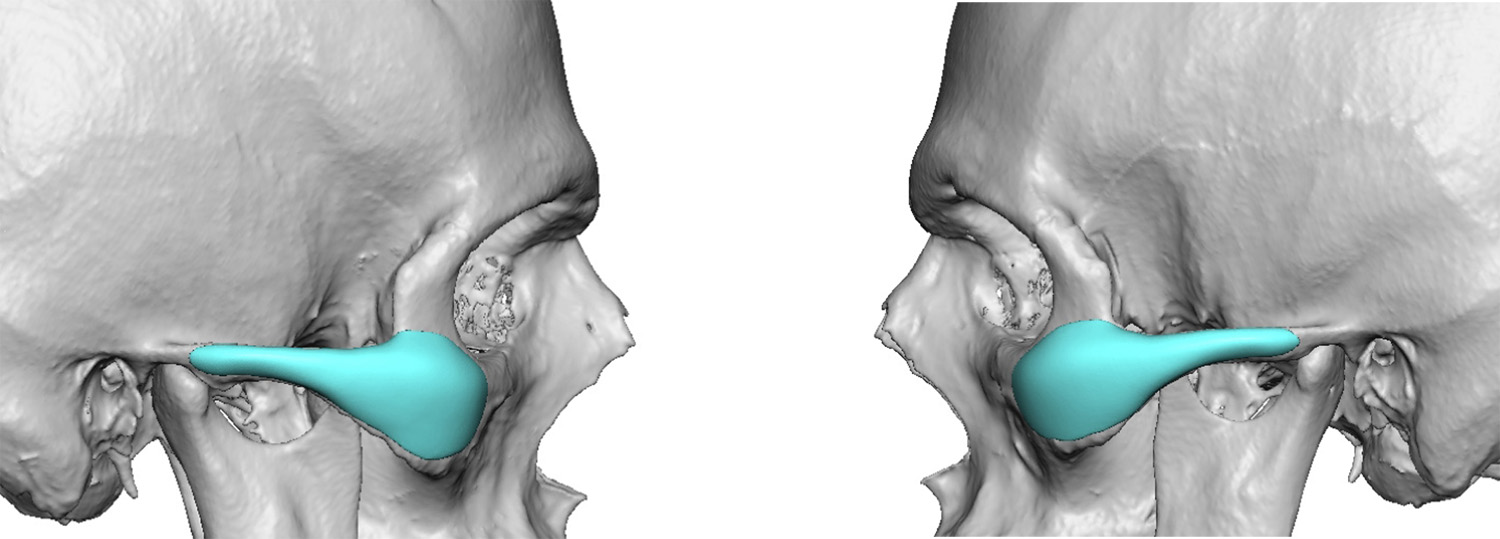
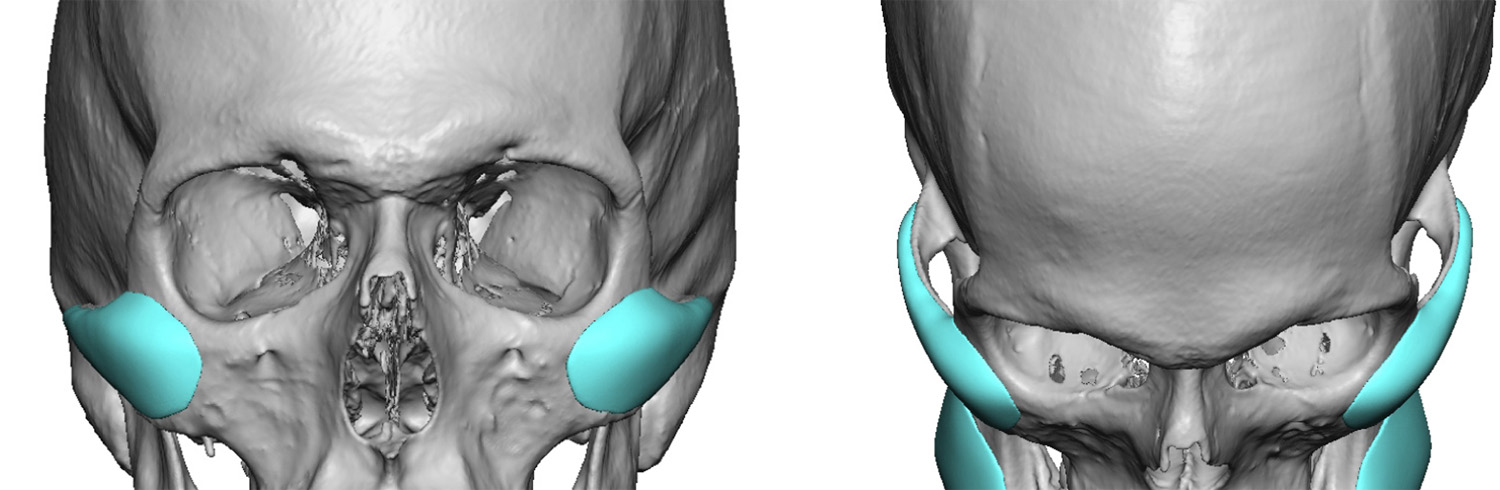 The high cheekbone or model cheek implant has its high point higher up on the cheekbone with a long posterior zygomatic arch extension. This helps to create an augmentation ridge from the cheekbone below the side of the eye back close to the temporal bone in front of the ear. This also gives a bit of vertical facial lengthening between the cheeks and the jawline helping to thin the face and give it some added angularity if one is thin enough.
The high cheekbone or model cheek implant has its high point higher up on the cheekbone with a long posterior zygomatic arch extension. This helps to create an augmentation ridge from the cheekbone below the side of the eye back close to the temporal bone in front of the ear. This also gives a bit of vertical facial lengthening between the cheeks and the jawline helping to thin the face and give it some added angularity if one is thin enough.
 Placement of the high cheek or model cheek implants largely differs only in the extent of the zygomatic arch dissection. It is needed to go all the way back along the zygomatic arch until it meets the temporal process just in front the temporomandibular joint. In this dissection it is important to stay right on the bone in the subperiosteal plane to avoid injuring the crossing frontal branch of the facial nerve.
Placement of the high cheek or model cheek implants largely differs only in the extent of the zygomatic arch dissection. It is needed to go all the way back along the zygomatic arch until it meets the temporal process just in front the temporomandibular joint. In this dissection it is important to stay right on the bone in the subperiosteal plane to avoid injuring the crossing frontal branch of the facial nerve.
Dr. Barry Eppley
Indianapolis, Indiana