

Cheek implants have been around for decades and have undergone an evolution of design changes. While initially developed as small oblong shapes to sit on top of the malar eminence, newer designs have incorporated the area under the malar eminence as well known as the submalar region. This has led to a variety of current shapes that include malar, submalar and combined malar-submalar (shell) styles, creating up to five different cheek implant options. (not to mention the various sizes of each style)
But careful analysis of the actual anatomy of the zygomatic complex (aka cheekbone) reveals that it does not match the shape of any current cheek implant. Structurally the cheekbone is fairly complex with a main body and three processes that articulate with other bones (frontal, temporal and maxillary) and has four borders. When the term ‘high cheekbones’ is used from an attractive and desirous facial beauty standpoint, this usually refers to more pronounced zygomatic arches or its posterior process. This causes a raised line along the sides of the face to appear which creates a distinct facial skeletal feature. This is often seen in fashion models in both men and women.
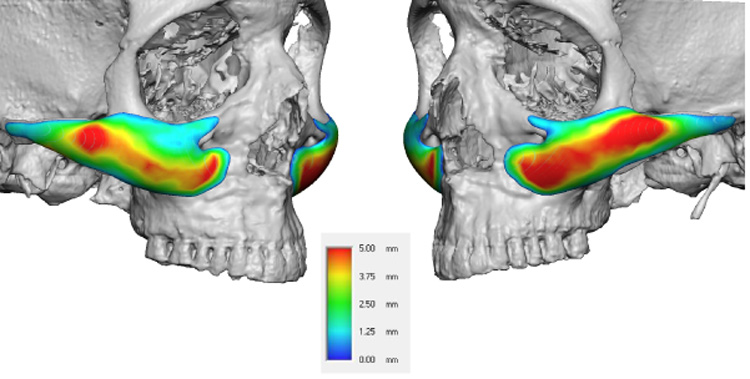 No performed cheek implant today truly creates the ‘model cheek’ look as they do not incorporate the zygomatic arch process as part of their design. To achieve this effect a special designed cheek implant is needed. It can have various anterior shapes but the key element in the extended posterior zygomatic arch process. This extension can go back all the way to the temporal region if desired. Besides creating the raised line back from the cheek it also creates a smoother and more blended flow up across the cheeks and back along the face rather than just a raised ‘bump’ over the cheekbone.
No performed cheek implant today truly creates the ‘model cheek’ look as they do not incorporate the zygomatic arch process as part of their design. To achieve this effect a special designed cheek implant is needed. It can have various anterior shapes but the key element in the extended posterior zygomatic arch process. This extension can go back all the way to the temporal region if desired. Besides creating the raised line back from the cheek it also creates a smoother and more blended flow up across the cheeks and back along the face rather than just a raised ‘bump’ over the cheekbone.

 This malar-arch cheek implant design is placed in the standard intraoral fashion through the mouth. Subperiosteal dissection is carried way back along the zygomatic arch. As long as one is right on the bone there is no danger of injury to the frontal branch of the facial nerve that crosses in the tissues above the posterior zygomatic arch. The length of the tail of the implant can be shortened based on the patient’s anatomy and aesthetic goals. Because the implant has a long surface area contact with the bone in a more horizontal orientation the risks of intraoperative implant malposition and postoperative migration (if screw fixation is not used) is greatly reduced.
This malar-arch cheek implant design is placed in the standard intraoral fashion through the mouth. Subperiosteal dissection is carried way back along the zygomatic arch. As long as one is right on the bone there is no danger of injury to the frontal branch of the facial nerve that crosses in the tissues above the posterior zygomatic arch. The length of the tail of the implant can be shortened based on the patient’s anatomy and aesthetic goals. Because the implant has a long surface area contact with the bone in a more horizontal orientation the risks of intraoperative implant malposition and postoperative migration (if screw fixation is not used) is greatly reduced.
The model cheek implant is a malar-arch design that adds a skeletal coverage area not previously seen in any previous midface implant. It creates the high cheekbone look that many younger patients today seek in with contemporary fashion and beauty trends.
Dr. Barry Eppley
Indianapolis, Indiana