

In rhinoplasty the only structure in the nose that is unaffected by osteocartilaginous maneuvers is the nostril base. When they remain wide, narrowing procedures can be done and are the last step in any rhinoplasty surgery. Alar base reduction is generally considered when the interalar distance exceeds the intercanthal distance. While often creating a minor change, nostril narrowing can be complementary to the rest of the rhinoplasty result.
Despite being a relatively small area, the history of nostril narrowing reveals a variety of surgical techniques. The original Weir procedure is based on an external alar wedge excision hiding the incision in the alar-facial groove. A subsequent technique avoided external scarring using an internal excision through the nostril base and vestibular floor. Later techniques incorporated both methods with external alar wedge resection combined with internal vestibular floor excision. A classification system based on the anatomy of the nostril widening and their objectives has been the most helpful and includes Type 1, alar wedge excision; Type 2, combined alar base and nostril sill excision; Type 3, sill excision alone; Type 4, combined alar base, nostril sill and nostril floor excision.
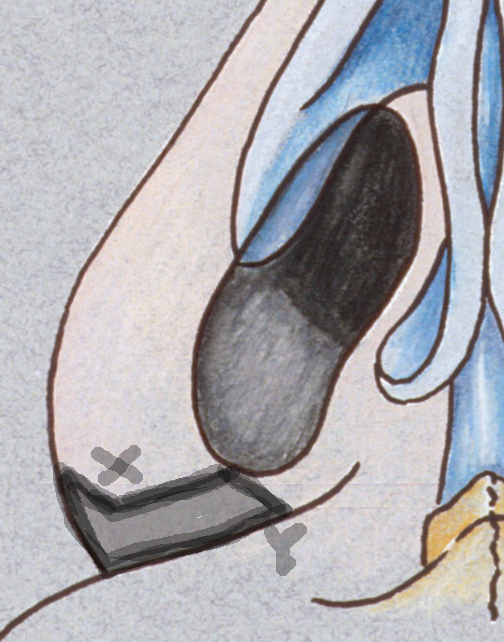 In the May 2018 issue of the Archives of Plastic Surgery journal an idea article was published entitled ‘A Refined Technique for Management of Nasal Flaring: The Quest for the Holy Grail of Alar Base Modification.’ In this paper the authors present a new method for reducing wide alar (nostril) flaring. What is different is that the incision is made in the alar-facial groove. The ‘V’ alar margin flap moves in and sits into the slot formed by the excision of the sill skin. In essence this is a transposition of the alar margin inward to the sill. This rotation of X point to be inserted into Y point moves the nostril in further than just sliding the remaining alar margin over to cover the sill excision. It also allows the curvatures of the incision along the existing curves of the ala with a concavo-convex skin wedge excision and creates a feeding notch for long-lasting results. The alar V-flap as it is moved inward maintains the normal alar curve, deepens the alar facial groove so the scar is better hidden, it avoids contraction of the resultant scar over the sill. Its use in 25 patients has proven to be successful.
In the May 2018 issue of the Archives of Plastic Surgery journal an idea article was published entitled ‘A Refined Technique for Management of Nasal Flaring: The Quest for the Holy Grail of Alar Base Modification.’ In this paper the authors present a new method for reducing wide alar (nostril) flaring. What is different is that the incision is made in the alar-facial groove. The ‘V’ alar margin flap moves in and sits into the slot formed by the excision of the sill skin. In essence this is a transposition of the alar margin inward to the sill. This rotation of X point to be inserted into Y point moves the nostril in further than just sliding the remaining alar margin over to cover the sill excision. It also allows the curvatures of the incision along the existing curves of the ala with a concavo-convex skin wedge excision and creates a feeding notch for long-lasting results. The alar V-flap as it is moved inward maintains the normal alar curve, deepens the alar facial groove so the scar is better hidden, it avoids contraction of the resultant scar over the sill. Its use in 25 patients has proven to be successful.
Nostril narrowing is a seemingly simple procedure and it is compared to the intricacies of most other rhinoplasty manuevers. However, it is prone to causing a variety of aesthetic alar base deformities such as visible scars, nostril asymmetry, overcorrection and undesired nostril shape distortions. The keys to nostril narrowing success is to not do it without a compelling reason, proper technique selection, careful marking and execution and conservative tissue excision.
Dr. Barry Eppley
Indianapolis, Indiana