


Reduction of wide cheeks can only be effectively achieved by moving the bone inward through osteotomies. Simply shaving the cheekbone is of limited value because it cannot adequately address the widest part of the cheekbone. Furthermore, the extensive soft tissue dissection required for shaving can lead to postoperative soft tissue sagging.
The Concept of Bone Bridge Repositioning
Cheekbone reduction osteotomies work on the concept of bridge repositioning. In patients with wide cheeks, the zygomatic arch — the widest part of the cheekbone — has increased outward convexity and sits further from the underlying temporal bones. This arch acts as a bridge between the anterior zygomatic major (the main body of the cheekbone) and the posterior zygomatic arch, which attaches to the temporal bone. By making precise cuts at both attachment points, the “bridge” can be repositioned inward, effectively reducing cheek width.
Osteotomy Techniques
While the cut at the posterior zygomatic arch is relatively straightforward (due to its thin structure), the anterior osteotomy can be performed using various techniques. The original approach — a vertical or vertical-oblique cut — has evolved into more advanced patterns, such as L-shaped osteotomies, to create a more three-dimensional effect.
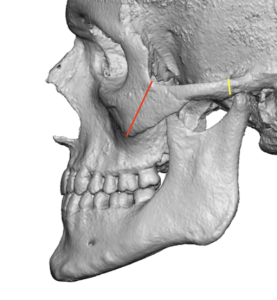 Despite these contemporary methods, the vertical oblique osteotomy can still produce excellent results when modified appropriately. The intraoral cut is made obliquely from the bottom of the posterior zygomatic buttress to just outside the lateral orbital wall (red line). The posterior zygomatic arch is mobilized (yellow line) with the traditional short vertical cut.
Despite these contemporary methods, the vertical oblique osteotomy can still produce excellent results when modified appropriately. The intraoral cut is made obliquely from the bottom of the posterior zygomatic buttress to just outside the lateral orbital wall (red line). The posterior zygomatic arch is mobilized (yellow line) with the traditional short vertical cut.
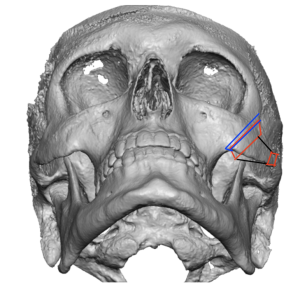 Because of the oblique angle through the bone, a step-off at the cut edges will occur, especially with larger reductions. This step-off is smoothed with a reciprocating saw using an angled cut to create a seamless transition between the two bone sides (red lines are the onward bone movement while the blue is the needed stepoff reduction)
Because of the oblique angle through the bone, a step-off at the cut edges will occur, especially with larger reductions. This step-off is smoothed with a reciprocating saw using an angled cut to create a seamless transition between the two bone sides (red lines are the onward bone movement while the blue is the needed stepoff reduction)
Posteriorly, as the arch bone is moved inward, it also slides backward, effectively locking the posterior cut end under the temporal process for added stability.
Importance of Fixation

 A significant advancement in cheekbone reduction surgery has been the routine use of plate and screw fixation — something often overlooked in procedures performed abroad. The oblique vertical osteotomy, in particular, requires fixation to maintain the horizontal alignment of the bone. An L-shaped plate is applied to ensure the repositioned bone remains stable and at the desired level.
A significant advancement in cheekbone reduction surgery has been the routine use of plate and screw fixation — something often overlooked in procedures performed abroad. The oblique vertical osteotomy, in particular, requires fixation to maintain the horizontal alignment of the bone. An L-shaped plate is applied to ensure the repositioned bone remains stable and at the desired level.
Outcomes
The modified intraoral vertical oblique osteotomy, when combined with a percutaneous posterior arch osteotomy, reliably achieves up to 8 mm of cheek width reduction per side — delivering predictable and aesthetically pleasing results.
Dr. Barry Eppley
World-Renowned Plastic Surgeon