


This is a technically delicate procedure because the oral commissure is a muscular convergence zone, not just a skin corner. Precision and conservative movement are critical.
Preoperative Planning
A. Measurement
- Determine desired amount of widening
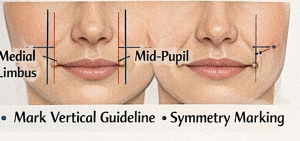
 Mark vertical reference lines from:
Mark vertical reference lines from:
- Medial limbus
- Mid-pupil (smile position)
- Avoid going lateral to mid-pupil in most aesthetic cases.
 Mark vertical reference lines from:
Mark vertical reference lines from:
B. Symmetry Marking
- Mark new commissure point bilaterally.
- Confirm in:
- Rest
- Natural smile
- Full smile
 Mark new commissure point bilaterally.
Mark new commissure point bilaterally.Even 1 mm asymmetry is noticeable.
C. Anesthesia
- Local infiltration with epinephrine
- Avoid over-distortion of tissues during injection
D. Mucosal Advancement Technique
Steps:
- Extend incision laterally from existing commissure through skin out to desired width mark
- Excise upper and lower triangular skin segments This leaves a skin defect into which the new mouth corner will move outinto it.
- Excise small wedge of exposed orbicularis muscle to make space for new commissure position
- Release and reposition commissure at skin-muscle ‘defect’
- Layered closure:
 Extend incision laterally from existing commissure through skin out to desired width mark
Extend incision laterally from existing commissure through skin out to desired width mark Excise upper and lower triangular skin segments This leaves a skin defect into which the new mouth corner will move outinto it.
Excise upper and lower triangular skin segments This leaves a skin defect into which the new mouth corner will move outinto it. Excise small wedge of exposed orbicularis muscle to make space for new commissure position
Excise small wedge of exposed orbicularis muscle to make space for new commissure position
-
- Deep absorbable sutures (muscle approximation)
- Mucosal closure
- Fine skin sutures at vermilion border
Key principle: recreate a natural commissure angle.
E. Postoperative Management
- Limit very wide mouth opening 10–14 days
- Scar management (silicone gel after epithelialize healing, usually 3 weeks)
Most Common Technical Errors
- Over-widening, leads to scar contraction which can pull corners medially and downward
- Failure to create muscle space for new commissure position
- Poor commissure angle recreation by not removing triangles of skin, leads to slit-like widening
Important Reality
This procedure may be technically small but aesthetically high-risk.The visible area is central to facial expression, so precision in execution is important to avoid asymmetries and/or increased scarring.
As a result
- prefer undercorrection
- Carefully counsel about visible scars and the potential need for secondary scar revision
How much widening is typically safe
In cosmetic mouth widening (lateral commissuroplasty), less is more.
Typical “Safe” Widening Range
- 4–5 mm per side (most common and safest range)
- Rarely 7 mm per side can be done but never more
That means total mouth width increase is usually 10mms or more
Why It’s Limited
The oral commissure is not just skin — it’s:
- A convergence point of multiple lip muscles
- A high-movement zone
- A tension-prone scar area
If widened too much:
- The corners can look pulled or unnatural
- The mouth may appear flat instead of curved
- Scars become visible when smiling
- Corners can drift downward over time from scar contracture
- “Joker” or “fish-mouth” appearance can occur
Even 1–2 mm makes a visible difference on the face.
How I Decide the Amount
It’s based on:
- Interpupillary distance (facial proportion reference)
- Existing commissure position relative to the medial limbus of the iris
- Smile dynamics
- Tissue laxity
- Patient ethnicity and lip thickness
As a general aesthetic guideline:
- The commissures ideally align near the mid-pupil or slightly medial at rest. Going lateral to the iris midline usually looks artificial.
- Recognize that the procedure is irreversible…you can always do more if desired
Dr Barry Eppley
Plastic Surgeon