

The corner of the mouth has relevance in aesthetic surgery due to its position and location. With aging or in some people who have it naturally, the mouth corners turn down. Treatments consist of Botox and filler injections or a surgical corner of the mouth lift. The mouth corner also establishes the width of the mouth with some affected by a small mouth (microstomia) or a large mouth (macrostomia) as defined by the horizontal commissure distance.
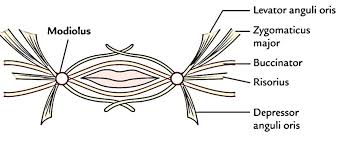 Besides being seen superficially as the junction of the lip vermilion and facial skin, underneath are a confluence of perioral muscles known as the modiolus. This is an anatomic term that describes a collection of intersecting muscles which include the orbicularis, buccinator, the levator and depressor anguli oris, zygomaticus major, risorius and the levator labii superioris. The modulus is important in mouth movements as well as for facial expressions.
Besides being seen superficially as the junction of the lip vermilion and facial skin, underneath are a confluence of perioral muscles known as the modiolus. This is an anatomic term that describes a collection of intersecting muscles which include the orbicularis, buccinator, the levator and depressor anguli oris, zygomaticus major, risorius and the levator labii superioris. The modulus is important in mouth movements as well as for facial expressions.
In the September 2018 issue of Plastic and Reconstructive Surgery an article was published entitled ‘Anatomical Characterization and Three-Dimensional Modeing of the Muscles at the Corner of the Mouth: An Iodine Staining Technique Based on Micro-Computed Tomography’. In this study the complicated muscular anatomy of the corner of the mouth was studied using iodine staining and micro-CT to evaluate the anatomy of the modiolus and surrounding muscles. They found that the muscle fibers of the modiolus runs in the direction of the muscle itself in a linear fashion. The pars marginalis of the orbiculares oris connects with the buccinator muscle, which accounts for why the corner of the mouth is oriented inward towards the oral cavity.
In corner of mouth lifts, a transpositional flap of vermilion is lifted upward to fill the gap left by the skin resection. In doing so it is important to release the underlying muscle and transpose an inferior muscle flap up to a more superior position to create a bit of a muscle lift or tightening as well. This means that the most superior part of the depressor angle iris is released and the orbiculares muscle sling is tightened.
 In mouth widening surgery the underlying muscles are released to allow the vermilion-skin mouth corner location to be moved laterally. This would be exclusively the pars marginalias of the orbiculares which would prevent an inward of the mouth corner after surgery, hopefully preventing relapse.
In mouth widening surgery the underlying muscles are released to allow the vermilion-skin mouth corner location to be moved laterally. This would be exclusively the pars marginalias of the orbiculares which would prevent an inward of the mouth corner after surgery, hopefully preventing relapse.
In mouth narrowing surgery the corner musculature is closed down by reapportion of the muscular sling. As the authors suggest separation of the orbicularis fibers into a marginalis and peripheralis flaps that are sutured with the upper muscle fibers on top of the lower fibers will help to form a more natural mouth corner overhang.
Dr. Barry Eppley
Indianapolis, Indiana