

The treatment of specific types of migraine headaches has been revolutionized by the use of Botox injections and migraine surgery. While not always producing a cure, both types of treatments can produce a significant reduction in symptoms that is sustainable. The basis for migraine surgery is essentially the deactivation of a trigger which for three out of the four established migraine sites involves sensory nerve decompression.
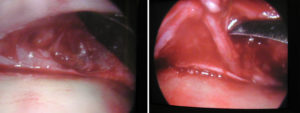 Frontal or forehead migraines can be triggered by compression of the superior divisions of the trigeminal nerve as they exit from the brow bones. The supraorbital and supratrochlear nerves can be compressed by muscle, vessels or the bone as its exits outward. Surgical decompression has been described using a superior endoscopic or an inferior transpalpebral (through the upper eyelid) approaches. Studies have shown that the endoscopic approach may produce better results than that of the transpalpebral technique.
Frontal or forehead migraines can be triggered by compression of the superior divisions of the trigeminal nerve as they exit from the brow bones. The supraorbital and supratrochlear nerves can be compressed by muscle, vessels or the bone as its exits outward. Surgical decompression has been described using a superior endoscopic or an inferior transpalpebral (through the upper eyelid) approaches. Studies have shown that the endoscopic approach may produce better results than that of the transpalpebral technique.
In the September 2016 issue of Plastic and Reconstructive Surgery, an article was published entitled ‘In-Depth Review of Symptoms, Triggers, and Surgical Deactivation of Frontal Migraine Headaches (Site I)’ In this paper 270 patients treated for frontal migraines who had at least one year followup were analyzed. A high percentage of patients (86%) as a successful outcome as determined by a greater than 50% improvement in the frontal-specific Migraine Headache Index. Over half of the patients (57%) reported a cure with complete elimination of their frontal migraines. Other symptoms beyond the headaches improved as well including blurred/double vision and visual auras. The most common complications were numbness of the nerve distribution which occurred in about one-third of the patients.
Frontal migraine surgery is associated with a high rate of symptom relief that is sustained for years after the procedure. It is not a perfect procedure as some patients don’t get complete relief and a few get little to no symptom improvement. One more recent anatomic understanding is the need to look for before whether the supraorbital nerve comes out from a notch in the brow bone or whether it exits through a completely encasing bony foramen. In such cases a foraminotomy is needed to release any potential bony compression on the nerve.
Dr. Barry Eppley
Indianapolis, Indiana