

 The hips have long been one of the main features of attractiveness for the female body. Having an outward curve of the hips is important as it creates a visual separation from the waist above it. Anthropometrically studies have shown that the relationship or ratio between the waist and hips (Waist-Hip Ratio, WHR), as measured by a linear line between their outer margins, is 0.6 to 0.7. This ratio indicates that the waist is also smaller in circumference than that of the hips.
The hips have long been one of the main features of attractiveness for the female body. Having an outward curve of the hips is important as it creates a visual separation from the waist above it. Anthropometrically studies have shown that the relationship or ratio between the waist and hips (Waist-Hip Ratio, WHR), as measured by a linear line between their outer margins, is 0.6 to 0.7. This ratio indicates that the waist is also smaller in circumference than that of the hips.
There are numerous conventional and commonly used surgeries to improve the WHR including liposuction and fat transfer. Liposuction attacks the waistline while fat transfer augments the buttocks and/or hips below it. This explains the success of BBL (Brazilian Butt Lift) surgery in which its diametric effect treats both sides of the WHR ratio. But not every patient qualifies or does well from these procedures particularly if they have little fat to harvest or have a narrow pelvic bone size/width.
To improve the WHR in thin or narrow waisted patients hip implants have been used with varying degrees of success. Conventional hip implants are placed below the iliac crest and over the hip dip area down into the upper lateral thigh. But a new procedure, known as Pelvic Plasty, provides a different approach to hip implants focusing on increasing pelvic bone width. In effect this is a skeletal expansion procedure using a specially designed titanium plate that its rigidly fixed to the iliac crest to achieve an increased pelvic width and an improved WHR.
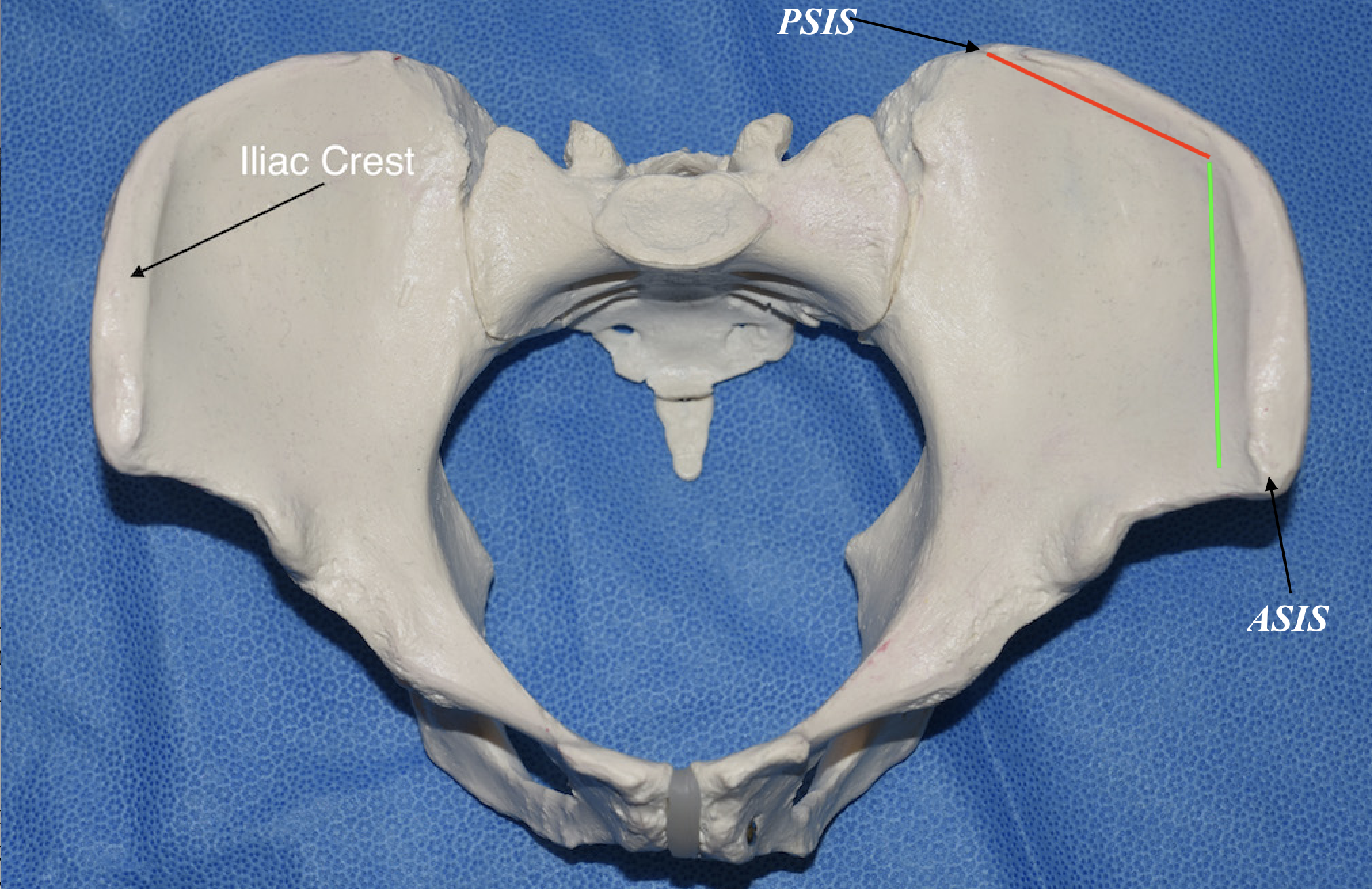
 To understand the placement of the Pelvic Plasty plate it is important to look at the anatomy of the iliac crest. The crest is the most superior part of the wing of the ilium and the most superolateral margin of the pelvis. It has a long curved length from front to back beginning at the anterior superior iliac spine (ASIS) to the posterior superior iliac spine (PSIS) and is close to the skin. As a result it can felt along its entire length. But as it relates to pelvic width, particularly increasing its width, the iliac crest has two halfs. The anterior half (green line) is what contributes to pelvic width. The posterior half (red line) markedly angles inward and does not contribute to pelvic width. Thus the effectiveness of any plate augmentation must have its greatest influence at the anterior half of the iliac crest.
To understand the placement of the Pelvic Plasty plate it is important to look at the anatomy of the iliac crest. The crest is the most superior part of the wing of the ilium and the most superolateral margin of the pelvis. It has a long curved length from front to back beginning at the anterior superior iliac spine (ASIS) to the posterior superior iliac spine (PSIS) and is close to the skin. As a result it can felt along its entire length. But as it relates to pelvic width, particularly increasing its width, the iliac crest has two halfs. The anterior half (green line) is what contributes to pelvic width. The posterior half (red line) markedly angles inward and does not contribute to pelvic width. Thus the effectiveness of any plate augmentation must have its greatest influence at the anterior half of the iliac crest.
While there are many muscles and ligaments that attached to the iliac crest at its outer edge or lip of the anterior half they are more limited. Near the ASIS is the tensor fascia lata and further back along the outer lip of the anterior half is the fascial attachments of the gluteus medius. There are abdominal muscles that attach to the crest but they are more on the inner lip.
There are no major blood vessels that cross over the anterior iliac crest. The nerves of relevance are the ilioinguinal and the lateral femoral cutaneous nerves. The ilioinguinal nerve of the lower abdominal wall, while crossing close to the ASIS, runs a bit more medial and anterior to it. The lateral femoral cutaneous nerve is the more recognized one in this area becomes of the well known nerve entrapment problem known as meralgiaparaesthetica causing chronic lateral thigh pain/numbness. While running closer to the ASIS it either crosses over to through the sartorius muscle which is a bit lower than the ASIS.
What the anatomy shows is increasing pelvic bone width must occur on the anterior half of the iliac crest. This is a safe anatomic area accessed through an anterior approach and has a low risk of causing any long term functional problem.
Dr. Barry Eppley
World-Renowned Plastic Surgeon