


Background: Midfacial width reduction/narrowing by cheekbone osteotomies is a well known surgical technique. While it has been popularized and is most commonly done in Asian patients, I have done it many times in other ethnicities as well. It is more about whether the cheekbone anatomy can be successfully changed to accomplish the patient’s goals of less wide cheekbones than being an isolated ethnic procedure.
The concept of cheekbone reduction is moving in the sides of the cheeks, which means the posterior cheekbone proper (zygomatic body) and the zygomatic arch behind it. This requites a front (anterior) and a back (posterior) osteotomies with plate fixation. While the shape of then bone cut anteriorly has numerous variations (due to the size of the bone), the posterior osteotomy is limited to a straight-line oblique cut given the small size of the bone. Such bone cuts allow the bone to moved/rotated inward thus narrowing the width of the cheek back along the line of the zygomatic arch.
Like all bilateral or facially paired surgical procedures, there is always the risk of postoperative asymmetry. This could be due to differences in the bone cuts, how much inward movement was done or a preoperative asymmetry that was not appreciated before surgery. All postoperative cheek asymmetries of concern should be evaluated with a 3D CT scan which will provide clear guidance as to the origin of the asymmetry and how to best secondarily treat it.
Case Study: This male had prior bilateral cheekbone reduction osteotomies. While the right side was perfect from the patient’s perspective, the left side still stuck out too far. He subsequently underwent multiple left-sided revisions in an attempt to get the ideal match to the other side, which will providing improvement, did not reach the level of the symmetry the patient desired.

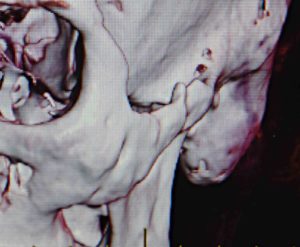 A 3D CT scan showed no appreciable differences in the position of either the anterior or posterior cheekbone segments. The posterior end of the zygomatic arch appeared more inward in the wider left than the right side. The scan indicated bony consolidation of the anterior osteotomy line.
A 3D CT scan showed no appreciable differences in the position of either the anterior or posterior cheekbone segments. The posterior end of the zygomatic arch appeared more inward in the wider left than the right side. The scan indicated bony consolidation of the anterior osteotomy line.
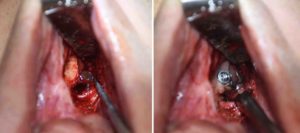 Under general anesthesia and through an intraoral approach the left anterior cheekbone osteotomy was recut and moved inward an additional 7mms. S percutaneous approach was done to move the end of the zygomatic arch further inward.
Under general anesthesia and through an intraoral approach the left anterior cheekbone osteotomy was recut and moved inward an additional 7mms. S percutaneous approach was done to move the end of the zygomatic arch further inward.
When asymmetry exists after cheekbone reduction osteotomies and the 3D CT scan shows symmetric bone positions, the dilemma becomes what to do. As there is no effective soft tissue reduction for the cheeks, all one can do is to try and move the bone further inward to compensate for soft tissue thickness differences.
Case Highlights:
1) Facial asymmetry after cheekbone reduction is best assessed with a 3D CT scan to understand the shape of the bone between the two sides.
2) Secondary cheekbone osteotomies can be done using the 3D CT scan to determine if anterior, posterior or both osteotomy locations are needed.
3) Postoperative facial asymmetries can exist even if the cheekbone shapes on both sides appear similar on the 3D CT scan.
Dr. Barry Eppley
Indianapolis, Indiana