

Background: It is said that no face is perfectly symmetric and some asymmetry is actually attractive. While these time honored statements are true, they really apply to facial asymmetries that are more of a modest nature. To those patients so affected with more significant facial asymmetries, they would undoubtably not agree. Thus improvements in many facial asymmetries are sought out by patients who see their issues as more than just slight in magnitude.
One of the most common parts of the face involved in asymmetry is the lower jaw. Being at the lower part of the face with a distinct separation from the neck, it is a facial area where asymmetries are easily seen. With a central chin and two paired sides of the jaw which initially develop independent of each other, there are lots of opportunities to have discrepancies in size and length. If the two sides of the lower jaw do not develop similarly a cant or asymmetry will be seen in the shape of the lower jaw.
Barring no need for occlusal adjustment, treatment of lower jaw asymmetry involves trying to equalize the shape of the bone on each side. This is judged by looking at the vertical length of the inferior border one each side as well as trying to equalize widths from the chin back to the jaw angles. The procedures needed depends on whether there is a ‘good’ side as the target or whether both sides need differential changes.
Case Study: This young male presenter with facial asymmetry that was most manifest in his lower jaw. He was also aware of some more mild asymmetry involving the right cheek bone and a lower corner of mouth on the right side as well. The lower jaw asymmetry was complex with a lower inferior border on the right side which extended to the chin, a shorter chin on the left side with a vertically longer jaw angle that was also less wide than the right side.
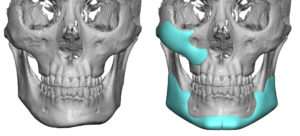
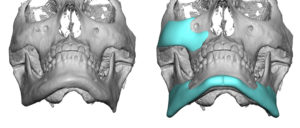
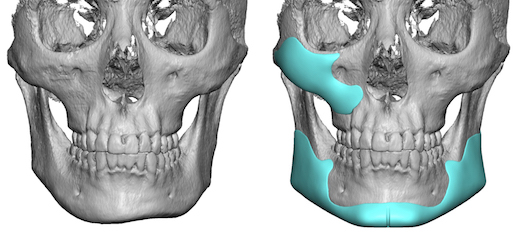
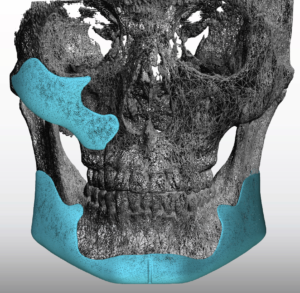
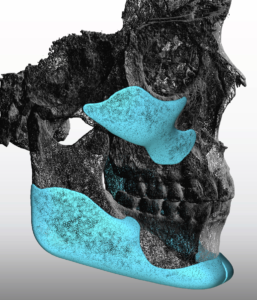
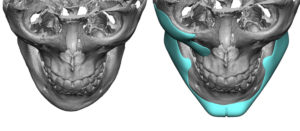 Given that the jawline goal was improved asymmetry and a more defined jawline as well, a custom jawline implant was designed. By setting the target outline around the perimeter first at the chin and jaw angles the implant thickness to the bone would create the asymmetry correction. This approach works if no part of the current jawline has adequate dimensions or is deficient throughout regardless of the asymmetry. During the same design process a right cheek-maxillary implant was created that mirrored the opposite aesthetically satisfactory left side.
Given that the jawline goal was improved asymmetry and a more defined jawline as well, a custom jawline implant was designed. By setting the target outline around the perimeter first at the chin and jaw angles the implant thickness to the bone would create the asymmetry correction. This approach works if no part of the current jawline has adequate dimensions or is deficient throughout regardless of the asymmetry. During the same design process a right cheek-maxillary implant was created that mirrored the opposite aesthetically satisfactory left side.
 Both the custom right cheek and jawline implant were implanted through intraoral incisions with the exception of an eternal submental incision.
Both the custom right cheek and jawline implant were implanted through intraoral incisions with the exception of an eternal submental incision.
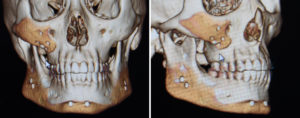
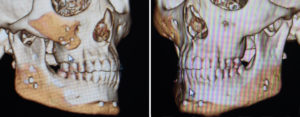 A postoperative 3D CT scan was done within days after surgery to use as a reference later when the swelling had largely subsided. At six weeks after surgery, while the patient had an uncomplicated recovery and improvements, some mild residual asymmetry of the chin and jaw angles persisted. The right cheek augmentation was acceptable and not a concern. Based on the 3D CT scan taken after surgery it showed almost perfect symmetry of the jawline implant placement, perhaps the right side being 1 or 2mms higher than the right side.
A postoperative 3D CT scan was done within days after surgery to use as a reference later when the swelling had largely subsided. At six weeks after surgery, while the patient had an uncomplicated recovery and improvements, some mild residual asymmetry of the chin and jaw angles persisted. The right cheek augmentation was acceptable and not a concern. Based on the 3D CT scan taken after surgery it showed almost perfect symmetry of the jawline implant placement, perhaps the right side being 1 or 2mms higher than the right side.
 While perfect facial symmetry is a good goal, most facial asymmetry surgeries realistically provide good improvement. But some asymmetries often persist. Provided that the custom implants are in good position, this leaves the variable of difference in soft tissue thickness as the potential cause. In this patient’s case it is undecided yet whether lowering the right side of the jawline will provide the desired improvements or whether a new custom jawline implant is the better answer.
While perfect facial symmetry is a good goal, most facial asymmetry surgeries realistically provide good improvement. But some asymmetries often persist. Provided that the custom implants are in good position, this leaves the variable of difference in soft tissue thickness as the potential cause. In this patient’s case it is undecided yet whether lowering the right side of the jawline will provide the desired improvements or whether a new custom jawline implant is the better answer.
Case Highlights:
1) Significant facial asymmetry is not rare and often involves the jawline.
2) The foundational approach to significant facial asymmetry is bone correction based on a 3D CT scan and custom designed implants if needed.
3) The success of custom jawline implants is based on the implant design, accuracy of implant placement and the contribution of the overlying soft tissues to the facial asymmetries seen.
Dr. Barry Eppley
Indianapolis, Indiana