

Background: The shape of the cheek is primarily controlled by the projection of the zygomatic body and the convexity of the zygomatic arch behind it. Given the length and potential variability of these combined zygomatic bone shapes, there is ample opportunity for one cheek to be different from the other. The degree of convexity or strength of the zygomatic arch is the main reason most cheeks are structurally different.
A 3D CT scan is the only definitive method to preoperatively determine the bony anatomy of the cheeks in cases of asymmetry. Trying to eyeball it or guess what makes up the structure of asymmetry from the outside is fraught with misinterpretations. Often the surgeon’s recommendations may be biased by the type of cheek procedure they know how to do or are most comfortable performing. This works satisfactorily when the actual problem coincides with the chosen procedure but not so well when it doesn’t.
Cheek reduction surgery consists of two basic procedures, cheekbone shaving and cheekbone osteotomies. Both offer some degree of cheek reduction but the most effective and widely used in aesthetic cheek narrowing surgery is the use of anterior body and posterior arch osteotomies. This affects the entire cheekbone and allows it to be moved inward with limited soft tissue stripping off the bone. Conversely shaving is limited only to the anterior portion of the main body of the cheek bone and requires wide elevation of soft tissues to do so.
 Case Study: This male had congenital right facial asymmetry of which one component of it was in the cheek. Even though he had a right facial asymmetry with the cheek more narrow on that side, his preference was for the smaller cheek side. The left cheek was wider and more pronounced. He had a prior history of a right cheek burring reduction which was done intraorally and at the main zygomatic body.
Case Study: This male had congenital right facial asymmetry of which one component of it was in the cheek. Even though he had a right facial asymmetry with the cheek more narrow on that side, his preference was for the smaller cheek side. The left cheek was wider and more pronounced. He had a prior history of a right cheek burring reduction which was done intraorally and at the main zygomatic body.
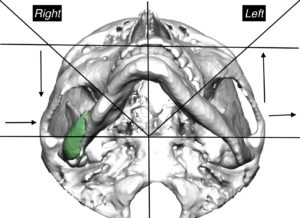
 A 3D CT scan showed that the residual cheek asymmetry was located at the posterior zygomatic arch-temporal process location. It also showed the very anterior location of the bone burring at the main zygomatic body.
A 3D CT scan showed that the residual cheek asymmetry was located at the posterior zygomatic arch-temporal process location. It also showed the very anterior location of the bone burring at the main zygomatic body.
 The new cheekbone reduction procedure would be a posterior osteotomy to reduce the prominence of the posterior zygomatic arch convexity. This would also require some bone burring reduction just behind the osteotomy line.
The new cheekbone reduction procedure would be a posterior osteotomy to reduce the prominence of the posterior zygomatic arch convexity. This would also require some bone burring reduction just behind the osteotomy line.
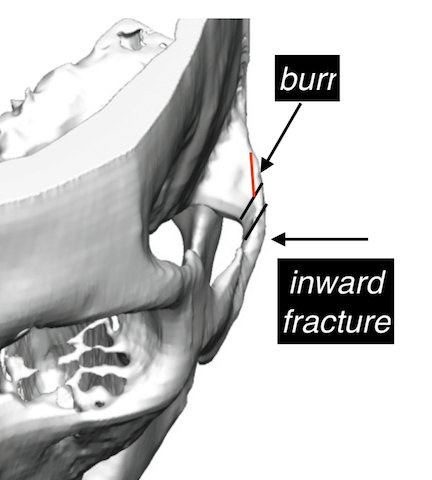
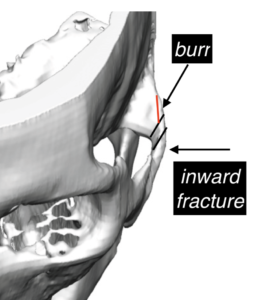
Under general anesthesia and through a percutaneous approach (10mm sideburn skin incision) an osteotome was used to create double cut in the posterior arch. The small intervening wedge of bone was removed which allowed the more anterior arch to be fractured inward. The zygomatic process of the temporal bone behind the bone cut was burred down to make it less projected.
In treating any form on facial asymmetry, the diagnostic process should include a 3D CT scan which provides the best insight into the differences between the two sides. Of all bony involvement in facial asymmetries, the cheek is a difficult area to fully assess externally because of its unique bony anatomy. and differing bone shapes. Just like in aesthetic cheekbone reductions the posterior arch osteotomy can be a useful technique in cheek asymmetry correction.
Case Highlights:
1) Cheek asymmetry can occur due to differences between the projection of the main body or the shape of the more posterior arch.
2) A 3D CT scan provides the best assessment of how the bony cheeks are different between the two sides.
3) Posterior cheek asymmetry is caused by the excessive projection of the zygomatic process of the temporal bone and the convexity of the posterior zygomatic arch.
4) The posterior zygomatic arch can be reduced through a percutaneous approach.
Dr. Barry Eppley
Indianapolis, Indiana