

Background: A custom jawline implant is designed with seven (7) specific dimensional components. Three of those dimensions relate to the more forward projecting part of the implant at the chin. While the chin constitutes less than 30% of the implant’s total surface area coverage it is the most valuable part of the implant due to its anterior visibility and the complete separation of the face from the neck that it creates.
When considering chin augmentation, whether it is part of a jawline implant or as just an isolated procedure, one has to assess the patient’s dimensional needs beyond that of the typical profile view. The only view assessment that can incorporate the dimensions of length, height and width is the three quarter view. But even in the two dimensions that the profile view provides, projection and height, the significance of verticality is frequently overlooked.
When vertical lengthening is needed using either a custom chin or jawline implant it is important to consider the soft tissue chin pad coverage. Unlike a sliding genioplasty or chin wing osteotomy where the inferior portion of the soft tissue chin pad remains attached and is always carried down with the bone movement, an implant detaches the complete soft tissue chin pad which then must be redraped over it during closure. The size of the horizontal and vertical implant augmentation has an impact on how successful that soft tissue redraping can be.

 Case Study: This male desired a jaw augmentation of which the chin was both horizontal and vertically deficient. This was determined by computer imaging that a 45 degree movement was needed for the best aesthetic chin projection.
Case Study: This male desired a jaw augmentation of which the chin was both horizontal and vertically deficient. This was determined by computer imaging that a 45 degree movement was needed for the best aesthetic chin projection.
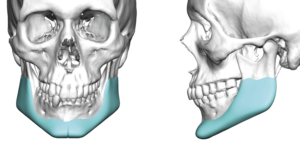
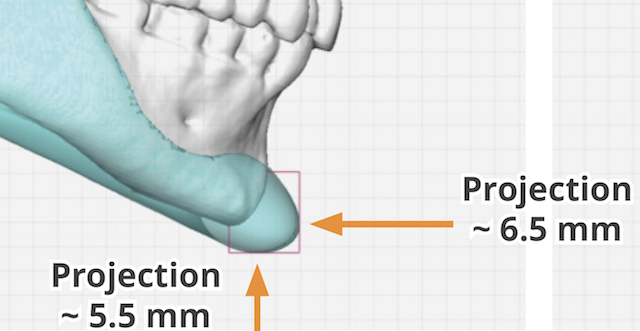
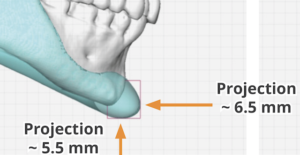
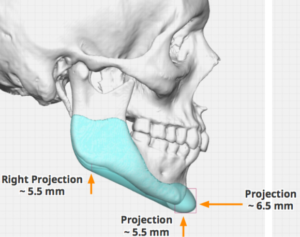 A custom jawline implant design was done that vertically lengthened the entire jawline from angle to chin. When combined with the horizontal augmentation of the chin the number 12 was obtained. My general rule for successful soft tissue chin redrawing over an implant in the chin is the combined horizontal and vertical change should not excess 12mms.
A custom jawline implant design was done that vertically lengthened the entire jawline from angle to chin. When combined with the horizontal augmentation of the chin the number 12 was obtained. My general rule for successful soft tissue chin redrawing over an implant in the chin is the combined horizontal and vertical change should not excess 12mms.

 Under general anesthesia the custom jawline implant was placed as a single piece through a submental incision. Posterior intraoral vestibular
Under general anesthesia the custom jawline implant was placed as a single piece through a submental incision. Posterior intraoral vestibular  incisions were used to create the jaw angle pocket needed and not secure that portion of the implant. A blue vertical marker is placed on the implant to help with midline alignment at the chin. The soft tissue chin pad was able to be successfully brought down over the implant edge and closed without undue tension.
incisions were used to create the jaw angle pocket needed and not secure that portion of the implant. A blue vertical marker is placed on the implant to help with midline alignment at the chin. The soft tissue chin pad was able to be successfully brought down over the implant edge and closed without undue tension.
While many think of large horizontal chin implant movements as not that soft tissue restrictive, adding a vertical component to the augmentation places greater stress on soft tissue redraping that one would think. Such vertical elongation often needs to be done at the expense of the horizontal change.
Case Highlights:
1) The chin component of a custom jawline implant must consider all three dimensions and not use the horizontal.
2) A combined horizontal and vertical increase or a 45 degree vector of augmentation is often needed for adequate lower facial profile improvement.
3) To ensure that the soft tissue chin pad can stretch back over an implant after being detached for implant placement the combined dimensional augmentation number in millimeters should not exceed twelve. (12)
Dr. Barry Eppley
Indianapolis, Indiana