


Background: Chin augmentation is primarily about an increase in the horizontal dimension. This is why the vast majority of before and after results seen are only shown in the profile view. It is also why most preoperative imaging is also done in the side view as well. While one can have a debate about how much horizontal increase any particular patient needs diagnosing a horizontal chin deficiency is well appreciated.
The one type of chin deficiency that is most frequently misdiagnosed is a vertical one. Surgeons frequently miss a vertical chin deficiency for two specific reasons. First it frequently is part of a horizontal deficiency as well of which total focus is directed to the correction of the horizontal component only. Secondly there has historically never been a standard chin implant whose intent was to try and create vertical chin length as a direct result of its design.
Vertical chin deficiencies can be diagnosed withs several physical findings. The lower facial proportions will be off with s short lower facial third. The distance between the lower lip and the bottom of the chin will just look disproportionately small. This is evident in any facial angle that is viewed. The chin will often look disproportionate to itself with it looking too wide. The soft tissue chin pad can take on several presentations. In younger patients it can look compressed and protrusive. In older patients it may appear as a form of chin ptosis with a soft tissue overhang. Most of the time the soft tissue chin pad is well adapted to the bone.
 A standard vertical lengthening chin implant does exist but few surgeons understand whom to use it on or how to use it to fit a particular patient’s aesthetic needs.
A standard vertical lengthening chin implant does exist but few surgeons understand whom to use it on or how to use it to fit a particular patient’s aesthetic needs.
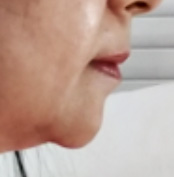
Case Study: This older female presented for chin augmentation. She felt her chin was short by horizontally and vertically. Her soft chin pad did have some overhang. She also had the presence of jowling with resultant prejowl notching or sulcus.

 Under general anesthesia and through a submental incision, wide subperiosteal undermining was done of the soft tissue chin pad as well as back along the jawline past the prejowl sulcus. A medium vertical lengthening chin implant was chosen, despite her small face, due to the length of the wings and the amount of vertical length it provides. While these dimensions were what was needed the chin implant was too round and wide. It was reshaped by reduction of the sides using a scalpel shaving technique.
Under general anesthesia and through a submental incision, wide subperiosteal undermining was done of the soft tissue chin pad as well as back along the jawline past the prejowl sulcus. A medium vertical lengthening chin implant was chosen, despite her small face, due to the length of the wings and the amount of vertical length it provides. While these dimensions were what was needed the chin implant was too round and wide. It was reshaped by reduction of the sides using a scalpel shaving technique.

 The implant was inserted, centered and then secured with single screw on the top edge of the implant. Like in any vertical lengthening chin implant there can be a relative soft tissue deficiency behind the vertical extension of the implant which should be filled in by advancing in soft tissue from the neck. This will make for a smooth submental line under the chin after closure.
The implant was inserted, centered and then secured with single screw on the top edge of the implant. Like in any vertical lengthening chin implant there can be a relative soft tissue deficiency behind the vertical extension of the implant which should be filled in by advancing in soft tissue from the neck. This will make for a smooth submental line under the chin after closure.

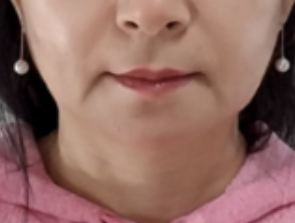
 Her one day after surgery results show the significant improvement in her chin shape with elimination of any soft tissue sagging.
Her one day after surgery results show the significant improvement in her chin shape with elimination of any soft tissue sagging.
Case Highlights:
1) The appearance of chin ptosis can occur because of inadequate vertical length of the underlying bone.
2) The vertically short chin creates as lower face disproportion.
3) The vertical lengthening chin implant provides a combined vertical and horizontal increase whose shape can be intraoperatively modified if needed.
Dr. Barry Eppley
Indianapolis, Indiana