


Background: The one primary feature that separates the male forehead from that of the female is the presence of visible brow bone mounds/protrusions. Males have these inferior forehead prominences and the suprabrow break above them that creates this uniquely male forehead shape. Occasionally some females will be seen with brow bone prominences but they are often much smaller in size.
While brow bone reduction surgery is well known in facial feminization, brow bone augmentation in facial masculinization is far less known. How to augment the brow bone poses challenges in how best to create the desired effect as well as can the augmentation be done with minimal scars. While in FFS surgery the use of frontal hairline and coronal scalp scars is how reductive forehead reshaping can only be performed the use of such incisions in male forehead augmentations is almost always aesthetically unacceptable.
Using a preformed implant made specifically for the patient and as well as using limited incisional access incisions are the two keys to making brow bone augmentation a procedure in which the benefits substantially exceed the tradeoffs.
Case Study: This male desired to masculinize his forehead through brow bone augmentation. Being able to do so through a custom implant approach was appealing as well as being to place it through a minimal scar technique.
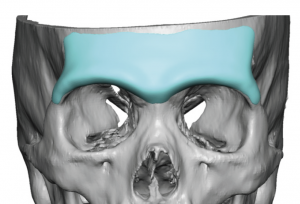
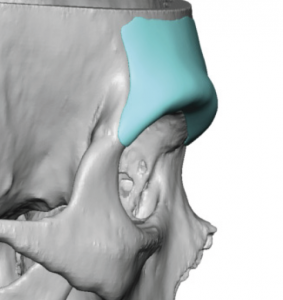 The key features on a custom brow bone implant include what brow bone surface areas should be covered (footprint), how much forward projection is adequate, how low on the brow bone should the projection be and what should the shape/dimensions of the brow bones be at it crosses between the bilateral fronto-zygomatic suture lines.
The key features on a custom brow bone implant include what brow bone surface areas should be covered (footprint), how much forward projection is adequate, how low on the brow bone should the projection be and what should the shape/dimensions of the brow bones be at it crosses between the bilateral fronto-zygomatic suture lines.

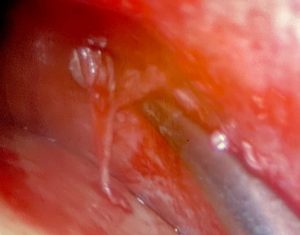 Under general anesthesia a small 3cm scalp was made behind the frontal hairline. Using an endoscope the release of the periosteal attachments across the brow bones was done. Because he had a high supraorbital nerve exit it was necessary release these small nerves at their foramen level.
Under general anesthesia a small 3cm scalp was made behind the frontal hairline. Using an endoscope the release of the periosteal attachments across the brow bones was done. Because he had a high supraorbital nerve exit it was necessary release these small nerves at their foramen level.

The custom brow bone implant was passed through the scalp incision perpendicular to its intended placement. It was then turned into proper orientation once inside the forehead pocket and slid down over the brow bones.

 Then two small scars near his eyelids, a right depressed scar lateral to the lateral canthus and a linear scar below the left eyebrow, were used for inferior access. Normally small incisions in the upper eyelid crease would be used so using the existing scars was opportunistic. The incisions allowed access to the lateral orbital rim to ensure the subperiosteal pocket was adequate for the ‘legs’ of the implant to be properly seated by pulling them down into place. This also allowed for screw fixation at the low lateral brow area.
Then two small scars near his eyelids, a right depressed scar lateral to the lateral canthus and a linear scar below the left eyebrow, were used for inferior access. Normally small incisions in the upper eyelid crease would be used so using the existing scars was opportunistic. The incisions allowed access to the lateral orbital rim to ensure the subperiosteal pocket was adequate for the ‘legs’ of the implant to be properly seated by pulling them down into place. This also allowed for screw fixation at the low lateral brow area.

 His intraoperative results showed the effects of the implant, producing an enhanced brow region and a forehead masculinizing effect.
His intraoperative results showed the effects of the implant, producing an enhanced brow region and a forehead masculinizing effect.
Of all the many different types of custom facial implants, brow bone implants are then only one whose placement can be aided by endoscopic visualization/dissection. The most important part of the procedure is to get the tissues released on the lower end of the brow bone (just inside the orbital rim) particularly down to the frontozygomatic suture on the upper lateral orbital rim. This is done in a more assured fashion by small incisions that allows direct visual access to the tails of the implant. Because of the thinness of these tails getting them low enough and in the proper position is the only way to ensure adequate implant placement. In certain types of brow bone implant designs the lower eyelid incisions may not he necessary but this is the exception and not the rule.
Case Highlights:
1) Custom brow bone implants can be most reliably placed in some patients through a triangulated small incisional technique.
2) The key in brow bone implant placement is to get it placed low enough on the existing brow bone where it can exert the best augmentation effect and avoid an unnatural look. No male patient wants higher brow bones.
3) Screw fixation is important as where the implant exerts its greater effect is where the greatest soft tissue recoil exists.
Dr. Barry Eppley
Indianapolis, Indiana