

Background: Clavicle fractures are a very common type of orthopedic bone injury with a reported occurrence of up to 4% of all fractures. Such fractures may be treated surgically with the placement of plates, screws and pins as well as non-surgically with post-injury shoulder immobilization slings/garments. With such a common type of bone injury it would be expected that it would inevitable that a patient seeking clavicle osteotomies for reductive shoulder reshaping would have a history of a clavicle fracture.
In patients with a prior history of a clavicle fracture a well healed fracture, even with some bone shape changes at the fracture site, does not preclude the ability to undergo a subsequent resection of bone length for shoulder narrowing. More relevantly, in fractures that have been repaired by hardware where is it located on the bone. Most clavicle fracture plates are quite long so they will need to be removed to perform osteotomies and then apply plates and screws to put the bone back together. However such fracture plates do not need to removed prior to the clavicle osteotomy surgery.
Most clavicle fracture repairs have very long surgical incisions in comparison to reduction osteotomies. Since this is the way the long fracture plate went in there is no reason not to use the full length of the incision which may benefit by scar revision anyway. Once the plate is exposed the type of screw heads used will be apparent. There are a wide variety of screw head shapes from the various manufacturers. While a crosshead pattern is most common there is no assurance that is what will be encountered. It is not possible to look at an X-ray and know what type of screw heads were used. Thus one should have a universal screw driver system available to be certain the hardware can be removed.
 Case Study: This female had a prior distal clavicle fracture and repair two years previously. She had a plate with four bicortical screws through the plate on each side of the fracture. She has a long scar over the length of the clavicle with the distal half being hyperytrophic. This was to be revised since the entire scar length was to be used. Given the long scar on the right side she wanted a similar scar length of the left side to match. (She planned on placing tattoos for scar camouflage later)
Case Study: This female had a prior distal clavicle fracture and repair two years previously. She had a plate with four bicortical screws through the plate on each side of the fracture. She has a long scar over the length of the clavicle with the distal half being hyperytrophic. This was to be revised since the entire scar length was to be used. Given the long scar on the right side she wanted a similar scar length of the left side to match. (She planned on placing tattoos for scar camouflage later)

 Under general anesthesia the right scar was excised over its full length and the hardware exposed. The screws were star-shaped so its was very fortunate that a universal screw drive system was made available for the surgery.
Under general anesthesia the right scar was excised over its full length and the hardware exposed. The screws were star-shaped so its was very fortunate that a universal screw drive system was made available for the surgery.

 The plate and 8 screws were removed. The underlying bone was well-healed, thick and covered with scar/capsule from the overlying plate.
The plate and 8 screws were removed. The underlying bone was well-healed, thick and covered with scar/capsule from the overlying plate.
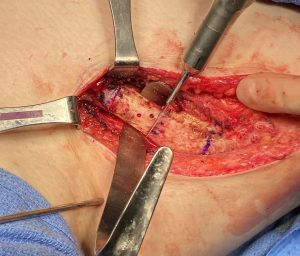 The scar tissue was removed from the bone and the planned osteotomy site marked. This incorporated a section of bone in which the previous medial screw of the plate were placed.
The scar tissue was removed from the bone and the planned osteotomy site marked. This incorporated a section of bone in which the previous medial screw of the plate were placed.
 A 2.75cm length of bone was removed and double plate fixation applied as the outer bone segment was brought in to put the two ends together.
A 2.75cm length of bone was removed and double plate fixation applied as the outer bone segment was brought in to put the two ends together.

 On the right side a similar length of bone was removed and plated back together. With sides were then closed in a multilayer fashion with resorbable sutures.
On the right side a similar length of bone was removed and plated back together. With sides were then closed in a multilayer fashion with resorbable sutures.
 It was noteworthy that the clavicle bone on the right side was 30% to 40% bigger in diameter from the non-fractured left side. Was this due to right hand dominance, the previous fracture or both?
It was noteworthy that the clavicle bone on the right side was 30% to 40% bigger in diameter from the non-fractured left side. Was this due to right hand dominance, the previous fracture or both?

 When seen several days after surgery the change in the shape of the shoulders was visually evident.
When seen several days after surgery the change in the shape of the shoulders was visually evident.
 Her postoperative x-ray showed good alignment and fixation of both reduced clavicles.
Her postoperative x-ray showed good alignment and fixation of both reduced clavicles.
Case Highlights:
1) Most prior clavicle fracture repairs by ORIF have hardware in place that will need to be removed to perform and fixate clavicle reduction osteotomies.
2) Such hardware does not need to be removed beforehand but can be done at the same time as the osteotomy. But one must be prepared with a universal screwdriver system.
3) The thickness of the bone on the fractured side may be thicker than the non-fractured side as a result of the healing from the injury.
Dr. Barry Eppley
World-Renowned Plastic Surgeon