

Background: The most effective method of aesthetic lower jaw augmentation is a custom jawline implant. Extending from one jaw angle to the other the entire inferolateral border of the jaw is augmented creating a connected and linear external lower facial enhancement. While tremendously effective there are limits in regards to the concept of implant load. This means the tolerance of the overlying soft tissues to tolerate the push of the underlying implant that is now positioned between it and the bone without creating complications.
This is most relevant in the front end of the lower jaw or the chin of a custom jawline implant. As a solitary projecting bony structure the chin pad is the tightest and least expansible soft tissue component of the entire jawline. There is a point when the size of the implant can make it difficult to close the incision without risk of postoperative dehiscence or increased risk of infection. This is no different than in chin augmentation alone when large chin changes are needed it is more achievable and safer to use an autologous method, the sliding genioplasty, which does not have the same soft tissue limitations as that of an implant.
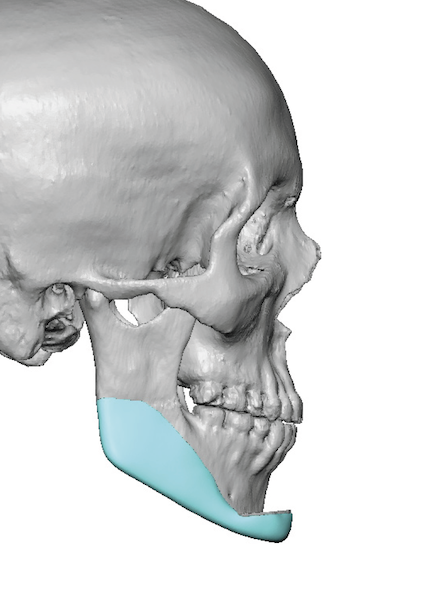
A sliding genioplasty can be combined with custom jaw implants to create a total jaw augmentation effect. Both the design of the bone cut and chin bone movement and the jaw implants are done on the patient’s 3D CT scan. Integrating the implant design into the sliding genioplasty allows for a smooth jawline effect. Making it blend together in surgery is a technical challenge but a surmountable and always a successful one.
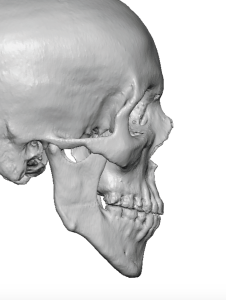
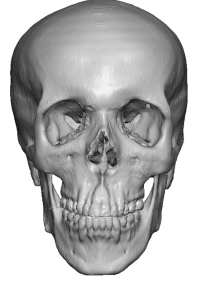 Case Study: This male had a very short but long chin and high jaw angles, an under rotated lower jaw deformity associated with inadequate growth of the mandibular ramus.
Case Study: This male had a very short but long chin and high jaw angles, an under rotated lower jaw deformity associated with inadequate growth of the mandibular ramus.
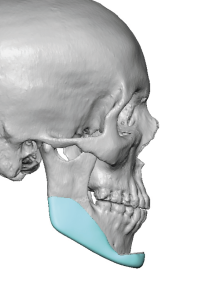
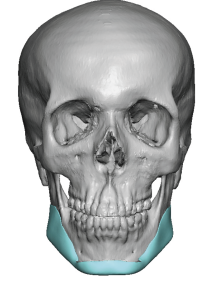 Based on preoperative computer imaging it was determined that the chin needed to come forward 12mms and up (vertically shorter) 4mms….a movement an implant would be stressed to make. Thus a sliding genioplasty was designed for this change with jaw implants for the rest of the jawline behind the chin. To derotate the jaw angles the implants provided vertical lengthening posteriorly and then merged with the designed sliding genioplasty movement.
Based on preoperative computer imaging it was determined that the chin needed to come forward 12mms and up (vertically shorter) 4mms….a movement an implant would be stressed to make. Thus a sliding genioplasty was designed for this change with jaw implants for the rest of the jawline behind the chin. To derotate the jaw angles the implants provided vertical lengthening posteriorly and then merged with the designed sliding genioplasty movement.

 The procedure was successfully performed merging the custom jaw implants with the sliding genioplasty movement.
The procedure was successfully performed merging the custom jaw implants with the sliding genioplasty movement.




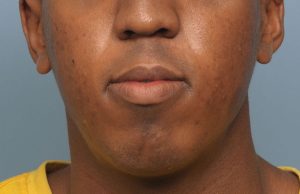
 When seen 4 months after the procedure the external effect of the jaw augmentation was just as impressive as the 3D CT scan designed surgery.
When seen 4 months after the procedure the external effect of the jaw augmentation was just as impressive as the 3D CT scan designed surgery.
While this combined bony and implant technique is the least performed method of aesthetic jaw augmentation and the most technically challenging to perform, it does have several advantages. It alleviates a large implant load off of the chin, reduces the risk of infection and avoids the need for any external incision.
Case Highlights:
1) One of the least common types of aesthetic jaw augmentation is combining a sliding genioplasty with custom jaw implants.
2) When the amount of chin dimensional change needed exceeds what can be safely tolerated for an implant the front end of the jaw augmentation needs to be done with a sliding genioplasty.
3) The combined autologous-alloplastic jaw augmentation can be done by a completely intraoral approach.
Dr. Barry Eppley
Indianapolis, Indiana