

Background: Facial implants are a common method used for permanent aesthetic augmentation. But the concept to grasp about their use is that is a reason that are available as off-the-shelf preformed implants….they are made for modest aesthetic concerns that can be improved by a single ‘spot’ augmentation. This is the role that standard cheek and chin implants, the most commonly used facial implants, perform in aesthetic surgery.
But when it comes to larger facial skeletal deficiencies, those have a more complex topography to them, an overall regional skeletal developmental hypoplasia, or when facial asymmetries exist, standard facial implants rarely provide an adequate result. This is were the role of custom facial implants offers superior because they fundamentally cover large surface areas of the involved bones which is really where the problem lies. It is a misconception that custom facial implants are bigger in size in terms of thickness, which may occasionally be true, but what they definitely are is bigger in bony surface area coverage.
This concept applies to the very common aesthetic orbitomalar deficiency. Usually associated with undereye hollows, the infraorbital rim is under developed in both height and projection. This extends around the corner of the cheek which has flatness and an inward rotation to the zygomatic body. It is important to recognize that it involves the zygomatic-orbital bone complex as an overall skeletal hypoplasia.
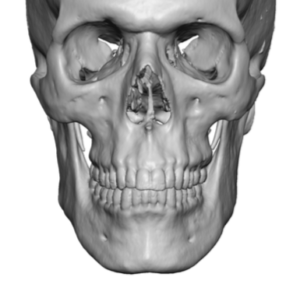
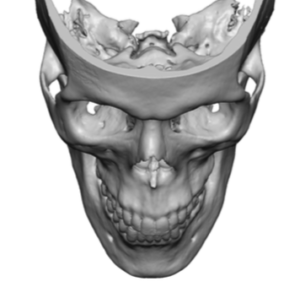 Case Study: This male wanted undereye and cheek augmentation to improve his narrow face, lack of cheek prominences and deep undereye hollows with pseudo fat herniation above the recessed infraorbital rims. His 3D CT scan demonstrated low infraorbital rims and inwardly rotated zygoma with lack of arch convexity. Hs overall facial shape frontally was vertically long and narrow.
Case Study: This male wanted undereye and cheek augmentation to improve his narrow face, lack of cheek prominences and deep undereye hollows with pseudo fat herniation above the recessed infraorbital rims. His 3D CT scan demonstrated low infraorbital rims and inwardly rotated zygoma with lack of arch convexity. Hs overall facial shape frontally was vertically long and narrow.
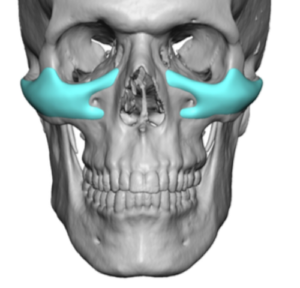
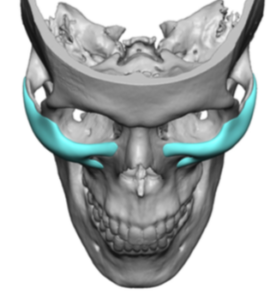
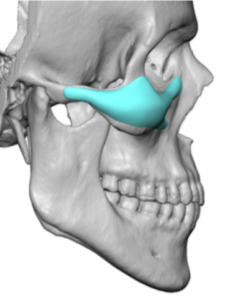 From the 3D CT scan custom infraorbital-malar implants were designed that extended from the nasal bones medially out to the end of the zygomatic arches. The infraorbital rim was raised by 2mms with similar projection. The cheek prominence at the curve (transition between orbit and zygoma) was 4mms. The patient preferred a result that was more modest than dramatic.
From the 3D CT scan custom infraorbital-malar implants were designed that extended from the nasal bones medially out to the end of the zygomatic arches. The infraorbital rim was raised by 2mms with similar projection. The cheek prominence at the curve (transition between orbit and zygoma) was 4mms. The patient preferred a result that was more modest than dramatic.
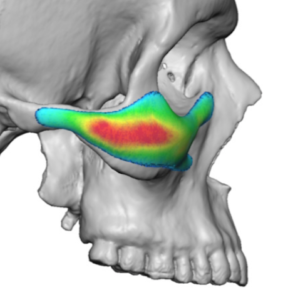
 The line of cheek augmentation could be appreciated in the color mapping of the implant’s thicknesses. A linear line of maximal thickness was seen around the level of the zygomatic arch creating the high cheekbone look. This can also be appreciated on the oblique or Ogee curve view.
The line of cheek augmentation could be appreciated in the color mapping of the implant’s thicknesses. A linear line of maximal thickness was seen around the level of the zygomatic arch creating the high cheekbone look. This can also be appreciated on the oblique or Ogee curve view.

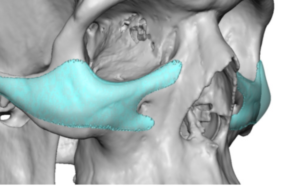
 Under general anesthesia the overlay of the implant on the midfacial augmentation area shows the extent of its coverage. Placed through a lower eyelid incision it was secured with a single microscrew to the cheekbone.
Under general anesthesia the overlay of the implant on the midfacial augmentation area shows the extent of its coverage. Placed through a lower eyelid incision it was secured with a single microscrew to the cheekbone.
![]() During closure the lower eyelid was elevated through the combined use of an Alloderm spacer graft and lateral canthoplasty.
During closure the lower eyelid was elevated through the combined use of an Alloderm spacer graft and lateral canthoplasty.
The scope of an aesthetic orbitomalar deficiency requires a custom implant approach in most cases. It is the only implant approach that cover the long horizontal line of bone augmentation that is needed. Associated with this bony deficiency is a lower eyelid roundness/sag particularly in the outer half of the lid. Since an eyelid incision is needed, the lower lid can be simultaneously leveled out with a combination of a lateral canthoplasty and a middle lamellar space graft.
Case Highlights:
1) Men who request correction of undereye hollows often have an associated narrow cheek width as well due to orbitomalar skeletal hypoplasia.
2) The custom infraorbital-malar implant creates a natural line of horizontal augmentation across the infraorbital rim out onto the zygomatic arch.
3) The long linear line of augmentation of a custom infraorbital-malar implant is best placed through a lower eyelid incision.
Dr. Barry Eppley
Indianapolis, Indiana