

Background: Excessive width or convexity of the side of the head is one of many head shape concerns. Generally it is preferred that the side of the head is straight rather than have any convexity. This becomes most relevant in men who have shorter hair styles where the shape of the side of the head is visible.
The side of the head is unique because, unlike the front, top and back of the head whose shape comes exclusively from that of bone, it has a major muscle component to its appearance. This is due to the large temporal muscle which extends from the side of the eye all the way to the back of the head. As the temporal muscle covers the side of the head it has various thicknesses which correspond to the shape of the underlying bone. The front or anterior part of the muscle is the thickest as the underlying bone is a deep concavity. As the temporal bone becomes a convexity further back at the side of the head the muscle becomes thinner over this more posterior part. While the temporal muscle does not really have an anterior and posterior belly, as it is all one continuous muscle, it is helpful in aesthetic skull reshaping surgery to think of it as such.
Removal of the posterior temporal muscle can be a very effective head width reduction procedure for those who have a convexity located above the ear. While many think the temporal bone is a major contributor to this shape it is not. The muscle makes a major contribution and its removal can also be done n a scarless fashion from an incision in the crease of the back of the ear.
But for some the excessive head width can also be located more towards the anterior part of the muscle which is not accessible from an incision behind the ear. Any reduction of the anterior temporal muscle fulness requires a direct incisional approach. Those who may benefit from anterior temporal reduction are those who have had a prior posterior temporal reduction and are looking for a more complete head widening effect or those with isolated anterior temporal fullness only.
 Case Study: This male had a prior history of a successful bilateral posterior temporal reduction. Six months later he decided that he also wanted to reduce the anterior temporal area as well. The fullness was anterior to the previous cut line of the posterior temporal muscle reduction.
Case Study: This male had a prior history of a successful bilateral posterior temporal reduction. Six months later he decided that he also wanted to reduce the anterior temporal area as well. The fullness was anterior to the previous cut line of the posterior temporal muscle reduction.

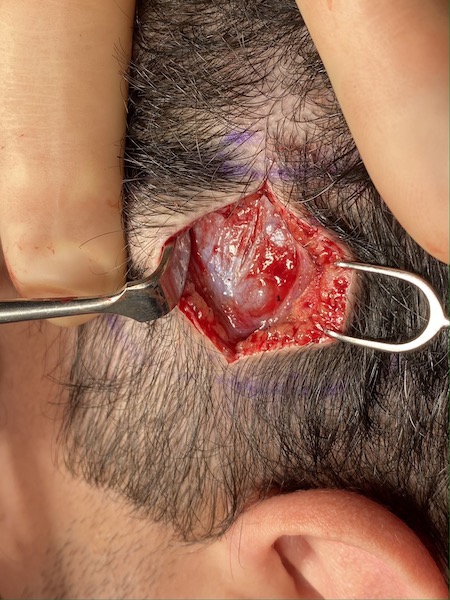
 Through a vertical incision down through the central area of the anterior temporal fullness, the muscle was exposed. Interestingly the prior edge of the muscle cut could be seen. While once that was a blunt thick edge of muscle after the prior procedure, it now had atrophied to a fine edge at the bone.
Through a vertical incision down through the central area of the anterior temporal fullness, the muscle was exposed. Interestingly the prior edge of the muscle cut could be seen. While once that was a blunt thick edge of muscle after the prior procedure, it now had atrophied to a fine edge at the bone.

 The exposed muscle was partially excised with cauterization of the remaining muscle bed. The scalp incision was then closed in two layers with resorbable sutures.
The exposed muscle was partially excised with cauterization of the remaining muscle bed. The scalp incision was then closed in two layers with resorbable sutures.
Unlike the posterior temporal muscle which can be reduced through a hidden incision behind the ear, this approach can not be used for the anterior temporal muscle. A direct approach is needed where partial thickness of the muscle can be directly excised. Cauterization not only controls bleeding but also helps the remaining muscle atrophy for further fullness reduction months after the surgery.
Case Highlights:
1) For a complete side of the head narrowing effect anterior temporal reduction can be done after posterior temporal reduction.
2) Anterior temporal reduction needs a direct approach through a small vertical incision overlying the area of greatest muscle protrusion.
3) In this case of anterior temporal reduction the prior cut edge of the muscle from the prior posterior temporal reduction could be seen.
Dr. Barry Eppley
Indianapolis, Indiana