


Background: The large temporal muscle occupies the entire side of the head even though its function is to contribute to movement of the lower jaw. Like the masseter muscle its masticatory activity can be a source of painful symptoms. Hyperactivity, nerve compression and vascular occlusion can be a source of such pain although the exact mechanism for masticatory pain, sometimes called myofascial pain dysfunction syndrome, is never precisely clear.
The treatment of masticatory muscle pain, while once the exclusive province of oral splints and TENS modalities, has now been aided considerably by the use of Botox injections. Reducing muscle activity by a direct impact on the neuromuscular junction can be an effective treatment even if its effects are not always permanent. If Botox injections are successful in reducing the size of the muscle along with improvement in pain, continuing Botox injections will continue to provide improvement. And it is possible that prolonged use of Botox may create a permanent subtotal or total pain relief.
But if repeated Botox injections are not desired despite improvement or numerous treatments have been done and the results remain short-lived, surgical treatment is many option. Borrowing from a temporal muscle removal procedure done for aesthetic purposes, where no negative functional effects have ever been seen, removal of the affected muscle can create a sustained reduction in pain and has the chance to be permanent.
Case Study: This male had a generalized feeling of tightness and discomfort around the sides of his head for years. He had received multiple sessions of Botox injections which reduced his pain as well as the size of his temporal muscles. He had gotten good improvement in the anterior portion of the muscle and their size had remained persistently reduced. His posterior temporal area while exhibiting some improvement as well still has some residual tightness particularly on the left side. He no longer wanted to continue with the Botox injections. Be examination his temporal muscles did not appear overly large and there was no strong bulge on biting down.

 Under general anesthesia the left temporal outline of the muscle to be removed was marked as well as the upper postauricular sulcus incision to access its removal. Once the sulcus incision was made dissection as carried down to the deep temporal fascia.
Under general anesthesia the left temporal outline of the muscle to be removed was marked as well as the upper postauricular sulcus incision to access its removal. Once the sulcus incision was made dissection as carried down to the deep temporal fascia.

 The posterior temporal muscle was released superiorly off of the overlying fascia as well as elevated off of the temporal bone along the external muscle markings.
The posterior temporal muscle was released superiorly off of the overlying fascia as well as elevated off of the temporal bone along the external muscle markings.

 A full thickness muscle cut was done with electrocautery at an angle from the top of the ear towards the forehead. The muscle was then released along the bony temporal line from front to back and removed through the incision.
A full thickness muscle cut was done with electrocautery at an angle from the top of the ear towards the forehead. The muscle was then released along the bony temporal line from front to back and removed through the incision.
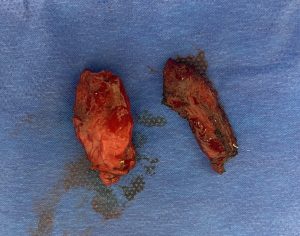
 More muscle was removed on the left side which had the greater residual symptoms. The postauricular incision were closed with dissolvable suture over the placement of a drain into the muscle removal sites.
More muscle was removed on the left side which had the greater residual symptoms. The postauricular incision were closed with dissolvable suture over the placement of a drain into the muscle removal sites.
While long term followup will confirm if his feelings of tightness are completely resolved it is anticipated that it will given the initial Botox injection results.
Key Points:
1) Temporal muscle removal can be done for the treatment of various pain conditions as well as for aesthetic enhancements.
2) A positive preoperative Botox test should be done first to determine that even a slight reduction in muscle provides some pain relief.
3) The location of the muscle pain should be primarily over the muscle located over the convex part of the temporal bone. (posterior temporal muscle)
Dr. Barry Eppley
World-Renowned Plastic Surgeon